

Iodine’s New Paradigm: More… or Less?
Alan Christianson, NMD
Iodine – not too much, not too little.
In Arizona, many retirees spend their summers elsewhere. To me, it marks the change of seasons to welcome my ‘snowbirds’ back in the fall and see them off in the spring.
Several years ago I had a kind gentleman return for the winter with new symptoms: watery diarrhea after every meal and a non-intentional tremor of his hand. The diarrhea started 3 or 4 months earlier, the tremor, more recently. Normally in excellent health, the patient joked about getting old and his body falling apart. He had his screening tests completed before I had heard about this. They were normal other than a suppressed TSH (thyroid-stimulating hormone) level. On his exam, I found several thyroid nodules that were not present the previous year and his heart rate was over 100 bpm.
An ultrasound along with second level thyroid tests diagnosed the patient with toxic multi-nodular goiter. In seniors, this is most common after high-dose iodine exposure such as in imaging contrast. I asked if he had had a CT or MRI done recently. He told me he did not but that he had been taking an iodine pill for 5 months. Apparently he was tested and found to be low in iodine and was now taking 1 tablet daily of a high-potency iodine/potassium iodide supplement providing 50,000 mcg of iodine.
Within several months I had roughly the same thing happen to 3 other patients, all on high-dose iodine, some based on testing, some not. One of these also had toxic multinodular goiter, one had Graves’ disease and one was hypothyroid secondary to Hashimoto’s thyroiditis. Since then, several more cases have come in with new thyroid disease after taking high-dose iodine.
Not all patients who take high-dose iodine will get thyroid disease and it is possible that some patients that I saw may have developed thyroid disease even if they weren’t on iodine. I have seen many other patients taking high-dose iodine with no apparent adverse effects.
Iodine in doses above physiologic requirements is the single best documented environmental toxin capable of inducing autoimmune thyroid disease (ATD).1
I had dimly been aware of iodine becoming a new topic at holistic conferences. A little digging quickly revealed that Guy Abraham, MD was the sole source of the new iodine paradigm.
Dr. Abraham collectively calls his work the ‘Iodine Project.’ The articles were originally published in the online quarterly journal The Original Internist, a non-peer reviewed journal circulating primarily to chiropractors. His ideas are mimicked nearly verbatum in books from Dr. David Brownstein (Iodine: Why You Need It, Why You Can’t Live Without It) and articles from Drs. Donald Miller and Jorge Flechas.
Over the next several months I read every word written by Dr. Abraham and his colleagues. I also read all of their references that were available. Most referred to their own statements from other sources. I also read everything I could find from every other source on human iodine requirements. My conclusion was quite clear: iodine at these new proposed doses was not justified and I have since counseled patients and peers against it.
Since these views on iodine are getting more pervasive, I felt compelled to share my findings and experiences in a broader forum.
The Iodine Project can be summarized as the following:2
- High-dose iodine helps conditions such as fibrocystic breast disease, therefore these doses are physiologically required.
- The Japanese consume much more iodine than Americans and have lower rates of thyroid disease and breast cancer.
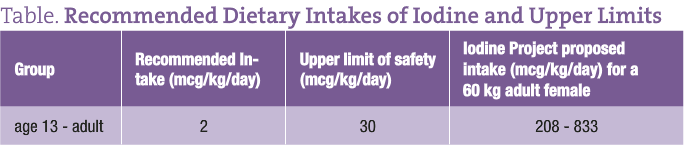
- Iodine status can be determined by 24-hour urine iodine levels following a 50,000 mcg oral dose. Those excreting a smaller fraction of the dose may have retained more iodine, therefore their bodies needed it.
- Adult humans need 12,500 – 50,000 mcg of iodine for good health.
- Iodine overdose is not a real phenomenon and the ‘Wolff-Chaikoff’ effect is a delusional construct resulting from “Iodophobic Bioterrorism.”
- The topsoil of the earth was divinely created 6000 years ago with an extremely high level of iodine, which was depleted by the flood of Noah. Human health has been poorer ever since.
- The current academic views on iodine are distorted by international foreign powers in order to make ‘zombies’ out of ‘Christian America.’
I imagine most who have entertained these ideas had no idea how radical some of the essential underlying concepts are. I could not make this stuff up. He rightfully states that the whole body of his work depends on points 6 and 7 to be valid.
These last points are so extreme, they deserve a few direct quotes from Dr. Abraham’s work:
“The theory of evolution does not offer an intellectually satisfying answer to this paradox. [humans needing iodine levels greatly in excess of what is found in sea water, as Dr. Abraham proposes]…Therefore, the original planet earth contained a topsoil rich in iodine, and all elements required for perfect health of Adam, Eve and their descendants….A sequence of events followed, culminating in the worldwide flood 4500 years ago. Following this episode, the receding waters washed away the topsoil with all its elements into oceans and seas. The new topsoil became deficient in iodine and most likely other essential elements, whose essentialities are still unknown.”3
“Iodine neglect in the 1930’s by thyroidologists progressed to medical iodophobia in the late 1940’s and early 1950’s. Following World War II, there was a systematic attempt to remove iodine from the food supply of Christian America. Iodophobic misinformation, well synchronized with the introduction of alternatives to iodine supplementation in medical practice, strongly suggest a well planned conspiracy by agents of foreign powers planted at strategic positions in academia and the regulatory agencies.”4
The Iodine Project claims that ‘iodophobia’ is part of a large conspiracy beginning in the 1930s. He discusses how in the 1960s Americans nearly became released from the “zombifying” clutches of iodophobia:
“In the early 1960’s, potassium iodate was added to bread as a dough conditioner….This was an oversight by the agents of foreign powers planted at strategic positions in academia and the regulatory agencies…. This amount of the dezombifier iodine in a major staple food of Christian America could not be tolerated for long.”4
My responses to the claims are as follows:
Research for Fibrocystic Breast Disease
Dr. Abraham states that his focus on iodine began after learning about the role of high-dose iodine in treating fibrocycstic breast disease in women.
The data that high-dose iodine can help fibrocystic breast disease is clear. Dr. Abraham is making the fallacy I have seen others make of confusing a useful property of a substance with its role as an essential element. Nutrients are cofactors for physiological functions in the body. Some also happen to have useful effects when used in doses well in excess of physiologic requirements.
Take niacin as a case in point. As adults we require only 14-18 mg of niacin to prevent us from developing pellagra, a potentially fatal niacin and protein deficiency disease. With a diet high in the amino acid tryptophan we can do fine on even lower amounts of niacin. It happens to be that doses of niacin 100-200 times this can act as a gentle HMG CoA reductase inhibitor.5 Yet these doses can cause maculopathy in up to 7% of adult males who take it.6 Those of you who use niacin in enough people have likely observed this reaction as I have.
Clearly, even though niacin may have useful properties in high doses, this does not mean that recommended intakes for all should be rewritten.
The majority of adults can tolerate intermittent high doses of iodine with no adverse effects. However long-term elevations, such as Abraham proposes, is different. Those who are low in iodine or who have positive thyroid antibodies can have adverse effects by raising their long-term intakes as little as 250 mcg/d.7
Those who are not deficient can manifest toxicity with as little as 600 mcg daily. The WHO (World Health Organization) has stated that 1000 mcg/d is a safe upper limit for most without thyroid antibodies. Thyroid antibodies are commonly present with normal thyroid function and can be found in up to 26% of the population.8 I did not find recommendations to pre-screen for antibodies prior to treatment in the Iodine Project.
Increased Intake, Increased Thyroid Problems?
Japanese, especially in coastal areas, do consume more iodine than Americans, but have higher rates of thyroid disease. Furthermore, their thyroid disease is highest in their areas of greatest iodine intake.9 Other populations whose iodine intakes vary from 100-200 mcg daily also have higher rates of thyroid disease.10
Japanese women used to have lower rates of breast cancer than American women. This difference declines as they adopt a Western diet. Researchers have shown strong dose-related increases in breast cancer among women from different nations related to dietary fat11; and inverse dose-related risks to intake of soy food and green tea.12,13
Validity of 24-Hour Loading Tests
I have been unable to find any sources outside of the Iodine Project pertaining to the validity of 24-hour loading tests, even after asking directly. Based on what we know about iodine, this test is not likely meaningful for the following reasons:
We excrete iodine in our urine but variable amounts leave though our bowels and sweat. Sudden large doses can result in fecal loss 400 fold above normal. It has been stated that unless fecal and urine levels of iodine are measured, urine is not an accurate biomarker when iodine intake is changed abruptly, such as after a loading dose.14
The CDC has also documented that a population’s 24-hour urinary iodine output levels are only meaningful when iodine intake has been steady for 6 months or greater. One does not reach steady state in 24 hours.15
Suggested Nutritional Intake Remains Low
Due to predictable thyroid toxicity, no nutritional organization has endorsed intakes of iodine above 600 mcg daily.
Iodized salt is ideally 1/10,000 potassium iodide, but third world countries in attempting to fortify salt often got the concentrations higher or lower. Since the WHO has carefully tracked these cases, we have extensive data regarding changes of iodine intake. Long-term intakes above 600 mcg/d routinely cause higher rates of thyroid disease including hypothyroidism and hyperthyroidism.16
Dronedarone is a nearly identical molecule to amiodarone minus the iodine. It shares the same effects and side effects of amiodarone with the exception of thyroid toxicity. Therefore it has been concluded that the thyrotoxic effects of amiodarone are attributable solely to the high iodine content.18Additional data on the long-term effects of high-dose iodine come from amiodarone usage. Each 200 mg tablet is roughly 75 mg of organic iodine, 8-12% of which is released as free iodide yielding an average net dose of 6-12.75 mg of iodine.
In a study of 182 patients taking amiodarone, 41% developed hypothyroidism over a 6-year period. Median time frame of onset for hypothyroidism was 21 months. After an average of 29 months, 59% of patients developed thyrotoxicosis. Note that some cases of thyrotoxicosis culminated in hypothyroidism so the groups did overlap.19
The Wolff-Chaikoff Effect
The Wolff-Chaikoff effect, AKA the ‘iodine escape mechanism,’ has been verified in vitro and in vivo and is present in all humans without exceptions or variations. Were such a ‘fuse’ not in place, normal variation of iodine intake could induce cardiotoxic hyperthyroidism. This effect is used when managing patients in a state of thyroid storm. One can suppress thyroid hormone synthesis with pharmacologic doses of iodine more quickly than with thionamide drugs due to the Wolff-Chaikoff effect.
This also enables a single high dose of potassium iodide (SSKI) to prevent thyroid cancer after radiation exposure. After taking enough SSKI, the thyroid iodine uptake is temporarily blocked due the Wolff-Chikoff effect. This prevents the thyroid from absorbing environmental radioactive iodine for roughly 3 weeks.
Religion vs Science
Religious belief, or lack thereof, is a personal matter. Yet modern medicine is based on biology and biology is based on evolution. If someone is unwilling to acknowledge the existence of planet earth prior to 6000 BC, then I see little basis on which to have a rational discussion regarding matters of science.
“Great Claims Require Great Evidence”
As NDs, we love to be the purveyors of arcane information that flies in the face of conventional wisdom. At least I know I do. Because of this eagerness, I think we can be vulnerable to embracing such ideas too uncritically. As Carl Sagan said, “Great claims require great evidence.”
The claim that the last 80 years of accumulated iodine knowledge duplicated from hundreds of researches in thousands of studies worldwide is all part of a ‘foreign conspiracy’ would require massive evidence, which I find lacking.
Fibrocystic breast disease can usually be treated with therapeutic doses of vitamin E, evening primrose oil, a diet high in fiber, and avoidance of methylxanthines (T. Hudson, ND, written communication, April 26, 2010). If considering iodine for resistant cases, pre-screen for antibodies and monitor thyroid function.
Breast cancer risk can be lowered by exercise, caloric balance, a low-fat diet, healthy use of soy and cruciferous veggies, and trading alcohol for tea.
Neither requires a treatment with a significant risk for generating thyroid disease. Finally, thyroid function does not improve when iodine consumption exceeds established ranges.
Given that risks of high-dose iodine are irrefutable, long-term intake should be kept at levels of roughly 150 mcg/d, although episodic intake of up to 1000 mcg is tolerable by most without thyroid antibodies.
For further reading:
- The Iodine Project in its entirety can be found at http://www.optimox.com/pics/Iodine/opt_Research_I.shtml
- A debate between Dr. Abraham and Dr. Alan Gaby can be found at the Townsend Letter archives: http://www.townsendletter.com/AugSept2005/gabyiodine0805.htm.
- From the Agency for Toxic Substances and Disease Registry (ATSDR) is over 200 pages of data summarizing human studies on toxicity of iodine: http://www.atsdr.cdc.gov/toxprofiles/tp158-c3.pdf; also 172 excellent references on iodine metabolism: http://www.atsdr.cdc.gov/toxprofiles/tp158-c9.pdf.
- CDC report on Iodine requirements in humans: http://www.cdc.gov/nutritionreport/part_4a.html.
- Iodine status worldwide from the WHO: http://www.who.int/vmnis/iodine/status/en/index.html.
- International Council for the Control of Iodine Deficiency Disorders, working to eliminate global iodine deficiency: http://www.iccidd.org/index.php.
 Alan Christianson, NMD was a member of the first graduating class of SCNM. His practice focus is on thyroid disease and natural endocrinology. He has completed The Complete Idiot’s Guide to Thyroid Disease for Penguin Press, and is rewriting the chapters on thyroid disease for the Textbook of Natural Medicine.
Alan Christianson, NMD was a member of the first graduating class of SCNM. His practice focus is on thyroid disease and natural endocrinology. He has completed The Complete Idiot’s Guide to Thyroid Disease for Penguin Press, and is rewriting the chapters on thyroid disease for the Textbook of Natural Medicine.
References
- Bahn RS. Immunogenetics, epigenetics and environmental triggers of autoimmune thyroid disorders. Paper presented at: Spring Meeting of the American Thyroid Association: Thyroid Disorders in the Era of Personalized Medicine; May 13-16, 2010; Minneapolis, MN.
- Iodine Publications. Optimox Corporation Web site. http://www.optimox.com/pics/Iodine/opt_Research_I.shtml. Accessed May 26, 2010.
- Abraham GE, Brownstein D. Validation of the orthoiodosupplementation program: a rebuttal of Dr. Gaby’s editorial on iodine. Optimox Corporation Web site. http://www.optimox.com/pics/Iodine/IOD-12/IOD_12.htm. Accessed May 26, 2010.
- Abraham GE. The history of iodine in medicine part III: thyroid fixation and medical iodophobia. Original Internist. 2006;13:71-78.
- Shah S, Ceska R. Efficacy and safety of extended-release niacin/laropiprant plus statin vs. doubling the dose of statin in patients with primary hypercholesterolaemia or mixed dyslipidaemia. Int J Clin Pract. 2010;64(6):727-738.
- Fraunfelder FW, Fraunfelder FT, Illingworth DR. Adverse ocular effects associated with niacin therapy. Br J Ophthalmol. 1995;79(1):54-56.
- Reinhardt W, Luster M, Rudorff KH, et al. Effect of small doses of iodine on thyroid function in patients with Hashimoto’s thyroiditis residing in an area of mild iodine deficiency. Eur J Endocrinol. 1998;139(1):23-28.
- Massoudi MS, Meilahn EN, Orchard TJ, et al. Prevalence of thyroid antibodies among healthy middle-aged women. Findings from the thyroid study in healthy women. Ann Epidemiol. 1995;5(3):229-233.
- Konno N, Makita H, Yuri K, Iizuka N, Kawasaki K. Association between dietary iodine intake and prevalence of subclinical hypothyroidism in the coastal regions of Japan. J Clin Endocrinol Metab. 1994;78(2):393-397.
- 10. Bülow Pedersen I, Knudsen N, Jørgensen T, Perrild H, Ovesen L, Laurberg P. Large differences in incidences of overt hyper- and hypothyroidism associated with a small difference in iodine intake: a prospective comparative register-based population survey. J Clin Endocrinol Metab. 2002;87(10):4462-4469.
- Gregorio DI, Emrich LJ, Graham S, Marshall JR, Nemoto T. Dietary fat consumption and survival among women with breast cancer. J Natl Cancer Inst. 1985;75(1):37-41.
- Leads from the MMWR. Ethnic differences in survival after diagnosis of breast cancer–Hawaii. JAMA. 1985;254(19):2728.
- Yamamoto S, Sobue T, Kobayashi M, Sasaki S, Tsugane S; Japan Public Health Center-Based Prospective Study on Cancer Cardiovascular Diseases Group. Soy, isoflavones, and breast cancer risk in Japan. J Natl Cancer Inst. 2003;95(12):906-913.
- Vought RL, London WT. Iodine intake and excretion in healthy nonhospitalized subjects. Am J Clin Nutr. 1964;15:124-132.
- Toxicological profile for iodine. Agency for Toxic Substances and Disease Registry Web site. http://www.atsdr.cdc.gov/toxprofiles/tp158.html. Published April 2004. Updated August 28, 2008. Accessed May 26, 2010.
- Roti E, Vagenakis AG. Effect of excess iodide: clinical aspects. In: Braverman LE, Utiger RD, eds. Werner & Ingbar’s the Thyroid: A Fundamental and Clinical Text. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2000:316-329.
- Fisher DA, Delange FM. Thyroid hormone and iodine requirements in man during brain development. In: Stanbury JB, Delange F, Dunn JT, Pandav CS, eds. Iodine in pregnancy. New Delhi: Oxford University Press; 1998:1-33.
- Han TS, Williams GR, Vanderpump MP. Benzofuran derivatives and the thyroid. Clin Endocrinol (Oxf). 2009;70(1):2-13.
- Martino E, Bartalena L, Bogazzi F, Braverman LE. The effects of amiodarone on the thyroid. Endocr Rev. 2001;22(2):240-254.







{kind=link}