Miriam Wheeler, ND, DHANP (DABHM)
A clinical case study demonstrating the successful eradication of Dientamoeba fragilis with Aloe socotrina in a lactating patient—offering a safe alternative to conventional antiparasitic medications.
Abstract
This case study details the treatment of a 32-year-old breastfeeding woman with an intestinal parasite, Dientamoeba fragilis, using the homeopathic remedy Aloe socotrina. The patient experienced complete resolution of symptoms without compromising breastfeeding safety, highlighting the value of classical homeopathy for sensitive patient populations.
Introduction
For patients who develop an acute infection while breastfeeding, choosing a safe and effective treatment option can often be challenging. It is not uncommon for our usual go-to antimicrobial herbs or even antibiotics and antiparasitic medications to lack safety data in this patient population. Furthermore, patients may feel apprehensive and uncomfortable with the potential risks the treatment may have on their child, even when the recommended treatment has been deemed safe to use by advisory boards or other regulatory agencies.
Based on the ultra-dilute nature of homeopathic medicines, the current body of evidence and historical uses of classical homeopathy suggest that homeopathic medicines are safe for use.1, 2 Even herbal medicines that are considered unsafe to use during lactation by LactMed (an online database managed by the National Library of Medicine), such as Arnica montana, are considered “usually safe during breastfeeding” when given as a homeopathic preparation.3 This case illustrates the important role homeopathy has when it comes to offering our patients safe and effective treatment options during all stages of life.
BACKGROUND & INITIAL CASE HISTORY:
LP, a 32-year-old female, presented with chief concerns of acute diarrhea and abdominal pain, which began approximately three weeks prior. Her obstetrician ordered a comprehensive stool analysis for her, which revealed the presence of Dientamoeba fragilis, a flagellate parasite that infects the large intestine.
Etiology was unknown, though the patient suspected that exposure occurred through her well water supply at home. She had begun using a filtration system since receiving the diagnosis. She also reported international travel to Uganda, Peru, Europe, and South Asia, though all of these trips occurred more than a year before the onset of symptoms. Since the patient was still breastfeeding her 18-month-old child, she was very apprehensive about beginning conventional or herbal anthelmintic treatments for this parasitic infection. She came to me seeking homeopathic treatment as a safe alternative.
She reported increased frequency of bowel movements (BMs) along with other changes to the stool itself since the onset of symptoms. She was currently having 3-7 BMs per day, increased from her typical 1-2 BMs per day. She stated the BMs could happen at any time of day, making planning her day difficult, though episodes tended to be worse later in the day (4-10 PM). Even while urinating, she often felt the urge to pass stool or gas. Since symptoms started, she experienced fecal urgency before BMs, which was accompanied by abdominal cramping and pain. The abdominal pain was episodic and located near the umbilicus. She described it as a crampy or gripping type of pain that came in waves. It was accompanied by diffuse abdominal bloating. The pain was worse before passing stool, at which time she also felt fecal urgency. She said that sometimes when she had the urge and pain, she was only able to pass gas, sometimes accompanied by mucus. However, passing gas and mucus provided temporary relief. The episodes of pain were often more intense from 4 to 10 PM. During waves of pain, she wanted to sit and avoid prolonged standing, which aggravated the pain.
After passing stool, she felt burning pain and itching at the anus. The increased frequency and urgency before a BM limited her productivity during the day and social life; she found herself worrying about being too far away from a toilet, which made it difficult to run errands and take care of household chores. She often passed a large amount of gas during the BMs. The increased gassiness was particularly distressing for her because it often felt as if stool might escape when passing gas, though she denied any episodes of fecal incontinence. The stool was at times “mushy” and in long pieces, but could also be small, soft balls. The stool was light to medium brown in color and usually covered in copious amounts of mucus. She had also begun seeing several drops of bright red blood in the toilet bowl after passing stool.
She had not tried applying hot or cold applications to the abdomen during waves of pain and was unsure what else affected the pain. She did not notice a correlation between the pain or frequency of BMs with what she ate or drank or when she ate/drank. She reported her appetite remained high, which she attributed to breastfeeding. She denied changes to thirst, urination, sleep, or energy since the onset of symptoms. She reported feeling frustrated by these symptoms, but denied changes to her mental-emotional state.
There was no pertinent psychosocial, past medical, or family history relevant to this acute case. She reported a clinical diagnosis of small internal hemorrhoids that had been asymptomatic until the onset of acute concerns. There was no other pertinent history upon review of systems. Physical examination was unremarkable, aside from tenderness to palpation of the abdomen diffusely.
LP was taking Thorne Basic Prenatal (1 capsule TID) and Nordic Naturals Pro DHA (1 capsule TID) but denied use of any prescribed or over-the-counter medications. She had not tried any treatments for her acute symptoms yet.
CASE ANALYSIS:
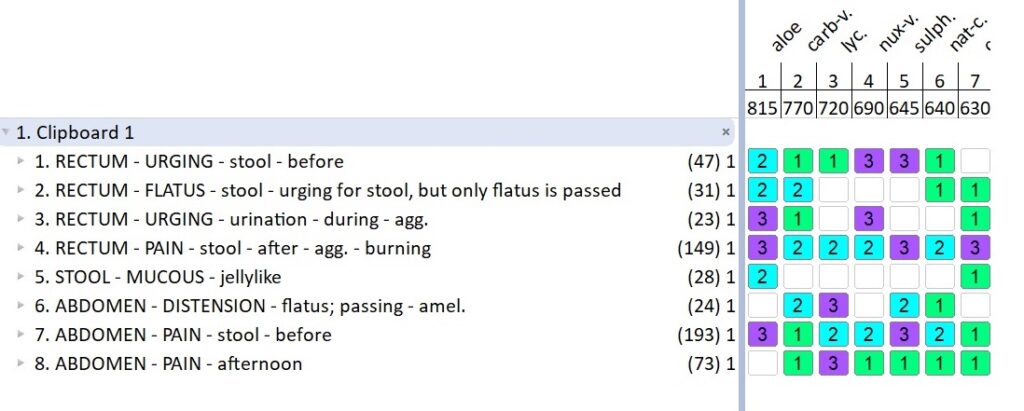
The bowel changes caused by the parasitic infection were identified as the primary concern of this case. My prescription was based on the repertorization using the RadarOpus computerized repertory, Synthesis Treasure Edition 2009V (Schroyens). The characteristic symptoms of the case matched in similarity with those highlighted below.
Aloe socotrina in Allen’s Encyclopædia of Pure Materia Medica4:
555. During slight distension of the abdomen and pleasant crawling of the bowels, three diarrhoeic stools; the last with burning in the rectum, haemorrhoidal pains, and much flatus (after seventeen hours) [1].
564. – * Burning at the anus after stool [27].
584. Blood passes after the stool [15].
604. Urgency to stool at times in the evening, which he can overcome (sixth day) [8].
605. – * Unusual urgency and haste to an evacuation [25].
606. – * He feels continually as if he thought to go to stool [8].
608. Frequent urgings (the first hours) [2].
610. Frequent inclination for a stool [13].
617. – * Urging and straining, yet only flatus passes off [11].
618. – * Compelled to stool, and only passage of flatus [24].
623. – * Urgency to stool, with passage of urine [8, 13].
634. – * Urgency and straining; then, after a few minutes, a liquid evacuation, with some blood and bloody mucus [20].
643. Urgency to stool in the afternoon and evening; at nine in the evening, a second indolent passage (fifth day) [8].
646. Griping before the diarrhea; tenesmus therewith [18].
647. Frequent griping before the stool; therewith, for the most part, flatulence, sometimes also straining at stool.
648. – * Fear lest a stool should escape with flatus [8].
649. – * While passing urine, a feeling as if some thin stool would escape with it [8].
650. – * Every time, on passing wind, the feeling as if some thin stool would escape with it (third day) [8].
679. – * Small, brownish, slimy, half-fluid stool [25].
411. – * Abdomen painful, especially in the umbilical region [7].
414. * A twisting and gripping pain in the upper abdomen, and around the umbilicus, compelling to sit bent up, which relieves; therewith, repeated urging to stool, but only flatus passes off, which is very offensive, and produces burning in the anus, with short relief from the pain (second day) [2].
415. Pinching and twisting pains around the umbilicus [27].
432. Flatulence moving about in the abdomen, which is distended (first day) [4].
465. – * Griping before going to stool [14].
467. In large doses, Aloes produces small stools, but very troublesome abdominal gripings (Hahnemann).
525. – * Only wind from an attempt to go to stool [4].
526. – * Much flatus and little feces [8].
527. – * Much wind with evening stool [11]; between the stools [8].
528. * Easy passage of flatus, with inclination as for a soft stool (5 P.M.) [11].
530. Very copious passage of flatus, during the whole night [11].
Aloe socotrina in Hering’s Guiding Symptoms of our Materia Medica5:
|| Stools are quite profuse with jelly-like lumps, and accompanied with wind. θ Colic.
In addition to Aloe, Sulphur and Lycopodium clavatum were also considered in this case. Sulphur covered the burning pain at the anus worse after passing stool, as well as the cramping pain in the abdomen before a BM. However, a keynote of Sulphur is diarrhea that is “more frequent in the morning”5 and which drives the patient “out of bed in the morning”5, and this timing did not match LP’s symptoms. LP reported the episodic abdominal pain that preceded a BM was worse from 4-10PM, and this timeframe made me consider Lycopodium clavatum, which is well known to produce symptoms that are aggravated from 4-8PM.5 LP also reported abdominal bloating that was ameliorated from passing flatus, another keynote of Lycopodium.5 However, the passing of only flatus when experiencing urging for stool and urging for stool while urinating were very reliable symptoms in this case, and particularly distressing for LP. Additionally, the passage of “jelly-like” mucus during BMs was also particularly characteristic in this case, which Aloe covered.5 Furthermore, while Aloe was not seen in the rubric for abdominal pain that is worse in the afternoon, Aloe does produce urging for BMs and increased flatulence in the afternoon and evening as seen above in the symptoms found in Allen’s Encyclopedia.4
I prescribed Aloe socotrina because it covered the most characteristic symptoms of the primary complaint along with the totality of symptoms, as Hahnemann instructed in Aphorism 153.
§153: “In this search for a homeopathic specific remedy, that is to say, in this comparison of the collective symptoms of the natural disease with the list of symptoms of known medicines, in order to find amongst these an artificial morbific agent corresponding by similarity to the disease to be cured, the more striking, singular, uncommon, and peculiar (characteristic) signs and symptoms of the case of disease are chiefly and most solely to be kept in view; for it is more particularly these that very similar ones in the list of symptoms of the selected medicine must correspond to, in order to constitute it the most suitable for effecting the cure. The more general and undefined symptoms: loss of appetite, headache, debility, restless sleep, discomfort, and so forth, demand but little attention when of that vague and indefinite character, if they cannot be more accurately described, as symptoms of such a general nature are observed in almost every disease and from almost every drug.”6
I instructed LP to dose Aloe socotrina 200c (3 dry pellets dissolved under the tongue) after each BM or episode of abdominal pain with fecal urgency (if only gas or mucus were passed). I had her dose in such a manner based on Aphorism 236.
§236: “The most appropriate and efficacious time for administering the medicine in these cases is immediately or very soon after the termination of the paroxysm, as soon as the patient has in some degree recovered from its effects; it has then time to effect all the changes in the organism requisite for the restoration of health, without any great disturbance or violent commotion, whereas the action of a medicine, be it ever so specifically appropriate, if given immediately before the paroxysm, coincides with the natural recurrence of the disease and causes such a reaction in the organism, such a violent contention, that an attack of that nature produces at the very least a great loss of strength, if it do not endanger life. But if the medicine be given immediately after the termination of the fit, that is to say, at the period when the apyretic interval has commenced and a long time before there are any preparations for the next paroxysm, then the vital force of the organism is in the best possible condition to allow itself to be quietly altered by the remedy, and thus restored to the healthy state.”6
CASE MANAGEMENT:
Check In (Day 4 of Treatment)
I called LP to check in, and she reported a 90% improvement in diarrhea and abdominal pain since beginning the Aloe 200c. She stated the fecal urgency had completely resolved, and she was only having 1-2 BMs per day again. She also stated that the abdominal pain that preceded a BM was quite mild now, and she was pleased by the significant improvements in both frequency and severity of symptoms. She denied experiencing an initial therapeutic aggravation and said, “All of my symptoms began to improve almost immediately!” Since she was reacting positively, I told her to continue dosing Aloe 200c (3 dry pellets dissolved under the tongue) after each BM.
Check In (Day 7)
I checked in with LP again a few days later. She reported she was continuing to see steady improvement and resolution of her symptoms. She stated the main symptoms at this time were the bloating and mild abdominal cramping at the umbilicus before passing stool. Occasionally, she still saw some mucus and a few drops of blood in the toilet after a BM. Since she was still reacting positively, I had her continue the same dosing schedule and instructed her to contact me if she felt she was approaching a plateau or if any symptoms began to relapse.
First Follow-Up (Week 4)
A couple of weeks later, she returned for a follow-up visit and reported that “everything is better.” She said the abdominal bloating and cramping pain had completely resolved. She was having 1-2 BMs per day. The stool was well-formed and easy to pass again without pain before or after a BM. The mucus and blood were still seen after a BM a couple of times a week, but it was less frequent than before. She denied any new symptoms or concerns. I had her continue dosing Aloe 200c after each BM.
Second Follow-Up (Week 8)
A month later, LP followed up and reported the bowel concerns had completely resolved. She was no longer seeing mucus and blood in the toilet after a BM. At this point, I had her discontinue the Aloe 200c since she no longer had symptoms from the parasitic infection. I ordered a repeat stool test to confirm eradication of the Dientamoeba fragilis. Results later revealed successful treatment, and there were no parasites or ova identified.
DISCUSSION & CONCLUSIONS:
This case demonstrates the successful homeopathic treatment of an intestinal parasitic infection. It was a particularly rewarding case to treat because this young mother’s symptoms were quite debilitating and embarrassing for her, and she desperately wanted to avoid taking anything that might have been unsafe to pass through her breastmilk. This case illustrates the effectiveness of dosing at the end of each paroxysm, allowing “the vital force of the organism (to be) in the best possible condition to allow itself to be quietly altered by the remedy, and thus restored to the healthy state.”6

Miriam Wheeler, ND, DHANP (DABHM), maintains a private practice in Phoenix, AZ, and also sees patients in California and Vermont via telehealth. She earned her Doctor of Naturopathic Medicine degree from Sonoran University of Health Sciences (formerly Southwest College of Naturopathic Medicine). She completed a two-year general medicine residency at Sonoran, followed by a third-year specialty residency in classical Hahnemannian homeopathy. She is board-certified as a homeopathic specialist in Arizona. She serves on the board of directors for Homeopathic Academy of Naturopathic Physicians and American Board of Homeopathic Medicine. She also serves as a guest lecturer at Sonoran University.
References
- Kirby BJ. Safety of homeopathic products. J R Soc Med. 2002;95(5):221-222. doi:10.1177/014107680209500501
- The Safety of Homeopathy. Report prepared by the European Council for Classical Homeopathy (ECCH). Jan 2009.
- LactMed – Drugs and Lactation Database. National Library of Medicine [database online]; 2024. Updated October 15, 2024. Accessed July 28, 2025. https://www.ncbi.nlm.nih.gov/books/NBK501828/
- Allen TF. Encyclopedia of Pure Materia Medica: A Record of the Positive Effects of Drugs upon the Healthy Human Organism [1874]. New Delhi: B. Jain Publishers reprint; 2000.
- Hering C. The Guiding Symptoms of our Materia Medica [1879]. New Delhi: B. Jain Publishers reprint; 1997.
- Hahnemann S. Organon of Medicine. 5th & 6th ed. Translated by Dudgeon RE [1833] and Hahnemann [1833]. New Delhi: B. Jain Publishers reprint; 1996.