

Focusing on the Thought Process : A Case of Post-traumatic Stress
Joseph Kellerstein, DC, ND
Jane was 14 years old. Like any young teen, she wanted to hang out with her friends. She lived in a smaller city some distance from Toronto but had the opportunity to get on a bus with some girls and hit the big city.
Once there she was introduced to a very “cool” crowd. Unfortunately, one night during a party there was trouble. Out of nowhere appeared a young man who was armed and very threatening. He robbed the group, holding Jane and others at gunpoint for several hours.
Jane has been a “nervous wreck” ever since. Where she once was an independent young lady, after the incident she was frightened of literally everything. She could not leave her parents’ house for one year following the incident. She was afraid to go to her bedroom to sleep, and preferred to sleep in the living room. Mornings seemed less anxiety laden.
The anxiety soon extended to worry regarding her health. At age 19, Jane lived as if she were dying, as if it were her last year. Leaving the house for any extended period of time would provoke an anxiety response. There was trembling, perspiration and a clouded head with headache.
Jane is now 29. She had been married once and is now in a committed relationship. She has one child.
Over the past year, Jane’s life and work have been generally stressful. No particular trauma. It seems that the panic that had subsided to a degree has re-emerged, and things have not felt right since. In fact, Jane had suicidal thoughts with intense and frequent panic. Jane is pessimistic, always thinking the worst in any situation. There is plenty of “what if” thinking.
Other symptoms:
- Especially while driving alone she is full of anxiety and negative thought (strong)
- She does not like public speaking
- There is a feeling of being hurried
- There is strong discomfort in busy places – anywhere she might be trapped
Jane consulted a local naturopath who prescribed Nux 30C as needed for the panic, which she used liberally for about one year, with some amelioration of the symptoms. There are headaches occurring daily at approximately 2 p.m. (shortly after taking her remedy). She expresses a strong desire for love and reassurance that she will seek from her partner. There is a fear of being alone (strong).
Over the past year, Jane has had several urinary tract infections that did not respond to antibiotics, ultimately resulting in chronic interstitial cystitis. There is frequent discomfort, but no discernable pattern of pain that can be reported.
Premenstrually there is sensitivity to being hot. When hot, she feels faint. There is a need for the cool, open air.
The most general relief is in the morning and things are worse in the evening.
Discussion
Now the “what if “ thinking, fear of going out and fear in potentially trapped areas might make us think of Argentum Nitricum, but there is no craving for sweet, which aggravates. There is no history of gastric trouble, and the remedy is absent in the rubric “morning amelioration.”
Pulsatilla clearly is the numeric leader (see Tables 1 and 2). The patient has a strong sensitivity to warm rooms before menses, and Pulsatilla is indeed characterized by this kind of thermal reaction. It is a leader for ailments from fright. “Consolation ameliorates” again is a strong feature.
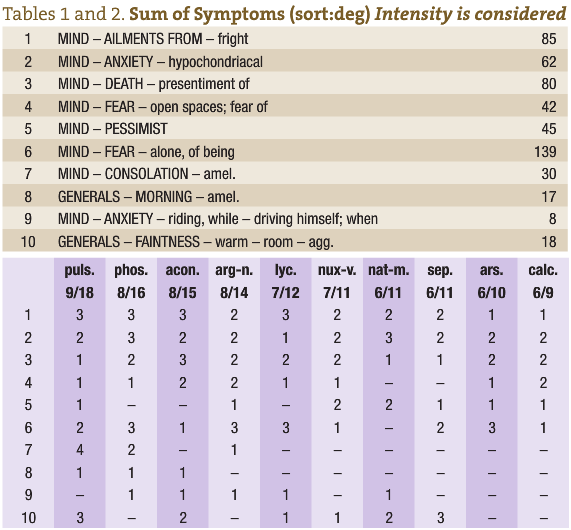
Phosphorus, too, is a strong contender. Phosphorus is a remedy characterized by “omnipresent anxiety”. It too has a strong presence in the rubric “ailments from fright.” For Phosphorus we would like to see a strong desire for cold drinks, which we don’t have. Thirst was unremarkable. This also goes for the thirstlessness of Pulsatilla. It was not there. The usual cravings found for Pulsatilla (creamy foods, fats … which aggravate) are not present. The cravings and aversions here were unremarkable. The time of aggravation of the headache was 2 p.m., which would support a prescription of Pulsatilla (Generalities afternoon 2 p.m.).
There are strong indications for all of these remedies. What is lacking in the previous two paragraphs, however, is directed thought. Many students think like this. From a random look at the top remedies in the repertorization, they arbitrarily debate back and forth regarding the merits of the remedies. Hahnemann gave us the Organon in order to help clarify the approach. Our guide into the forest of Materia Medica is the genius of the case. The genius of the case is the minimum syndrome of maximum value. We carefully question and sculpt out a case so that we have accurately traced the elements of the patient’s experience of disease that have been most consistent, emphatic and characterizing. The next order of business is to select the most characterizing elements and order them so as to truly be a guiding compass in this quest of remedial discovery.
What is most daunting about this is that we hold ourselves vulnerable to being wrong, and so we avoid the peril. Oh well, let’s jump in.
Characterizing Elements
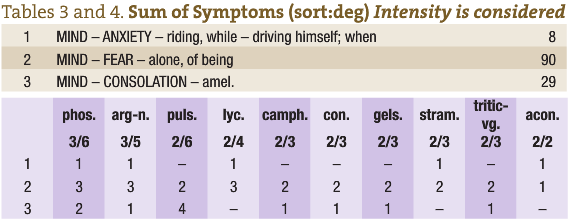 In this case I decided that the strongest and most characteristic symptoms pertaining to the case were, in order:
In this case I decided that the strongest and most characteristic symptoms pertaining to the case were, in order:
- The anxiety and bad thoughts while driving alone
- Fear of being alone
- The need for reassurance (consolation)
Again, Argentum and Phosphorus now vie for position, but the general amelioration was especially in the morning, so the choice here goes to Phosphorus (see Tables 3 and 4).
It may be argued that the most omnipresent symptom was the pessimism, which Phosphorus does not seem to have. This troubled me, so I consulted the Complete Repertory to discover that an author had added it:
MIND; PESSIMIST (SI-794) (Brooding) (Complaining) (Cowardice) (Delusions; fail – succeed – wrong) (Despair) (Discouraged) (Doubtful; recovery) (Hopeless) (Lamenting) (Loathing; life, of) (Succeeds, never) (Weary of life) (42) : agav-t.JulR, Alum.MoBF, anac.Her, arg-n.MoBF, ars.GalP, aur., bar-c.GalP, but-ac.MoBF, calc., calc-f.AlnE, carb-an.AlnE, caust.GalP, cecr.JulR, cic.KentC, cimic.MoBF, ferr-p.AlnE, fl-ac.AlnE, gad.AlnE, germ.ShrD, graph.AlnE, halo.JulR, hyos.GalP, kali-p.MoBF, lach.GalP, morph.AlnE, nat-c.AlnE, nat-m.MoBF, nit-ac.AlnE, nux-v.GalP, op.AlnE, pers.JulR, phos.MoBF, psor.Schm, puls.MoBF, sec.AlnE, sep.GalP, stann.JulR, staph.MoBF, ther.MoBF, thuj.AlnE, vip-a.JulR, wies.AlnE
Phosphorus 200 was given, and Jane has done very well in both the anxiety and the bladder symptoms.
My purpose here was not to present this case-in-progress as a cured case, but rather to render transparent a thought process given to us by Hahnemann. In Aph. 153, he declares that the homeopathic art is in the comparison of the case with materia medica. This ordering process gives a needed basis to that art.
 Joe Kellerstein, DC, ND graduated as a chiropractor in 1980 and as an ND in 1984. He graduated with a specialty in homeopathy from the Canadian Academy for Homeopathy, and subsequently lectured there for two years. He also lectured in homeopathy for several years at CCNM; for eight years at the Toronto School of Homeopathic Medicine; and for two years at the British Institute for Homeopathy. Dr. Kellerstein’s mission is the exploration of natural medicine in a holistic context, especially homeopathy and facilitating the experience of healing in clients.
Joe Kellerstein, DC, ND graduated as a chiropractor in 1980 and as an ND in 1984. He graduated with a specialty in homeopathy from the Canadian Academy for Homeopathy, and subsequently lectured there for two years. He also lectured in homeopathy for several years at CCNM; for eight years at the Toronto School of Homeopathic Medicine; and for two years at the British Institute for Homeopathy. Dr. Kellerstein’s mission is the exploration of natural medicine in a holistic context, especially homeopathy and facilitating the experience of healing in clients.







{kind=link}