

Inositol for PCOS
Megan Chmelik
Jacob Schor, ND, FABNO
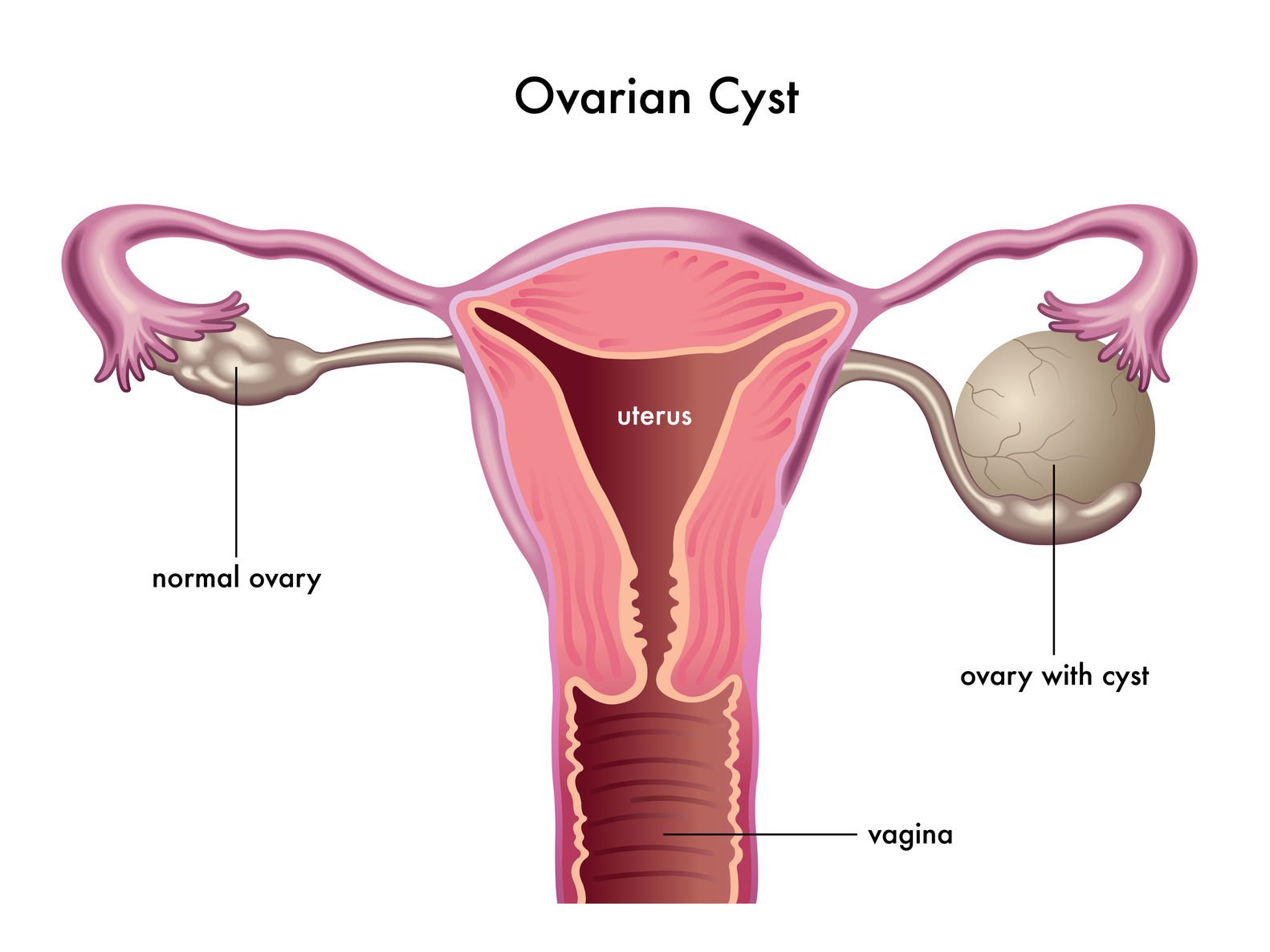
Polycystic ovarian syndrome (PCOS), categorized by irregular menstruation, ovarian cysts, and excessive androgen levels, is an increasingly common endocrine disorder affecting 4-12% of women of childbearing age.1 Often thought of as a modern disease, where factors such as poor diet, inactivity, and stress increase its severity and prevalence, the genetic origins of PCOS likely date back to the Paleolithic era. Historic figures in medicine describe symptom pictures that we easily recognize as PCOS:
According to Hippocrates,
…those women whose menstruation is less than three days or is meager, are robust, with a healthy complexion and a masculine appearance; yet they are not concerned about bearing children nor do they become pregnant.2
Moses Maimonides (1135-1204 AD) also noted that…
…there are women whose skin is dry and hard, and whose nature resembles the nature of a man. However, if any woman’s nature tends to be transformed to the nature of a man, this does not arise from medications, but is caused by heavy menstrual activity.3
PCOS: Historically vs Modern Day
Thus, it would appear that the symptom picture we now call PCOS has been around for a long time. It is curious that the PCOS genotype has survived all this time, as one might assume that a condition that decreases likelihood of reproductive success would disappear over time. The explanation perhaps lies in the concept that the PCOS “gene” is considered thrifty, allowing those with PCOS to survive on fewer calories.4 Having a sturdier frame and lower energy needs due to insulin resistance could be beneficial during times of famine.5 It may be that in an earlier, more primitive world where energy intake was frequently limited and energy expenditure was often high, that the PCOS genotype did not impact fertility as much as it does now.
In today’s world, having PCOS is not considered quite as advantageous as it was in the Stone Age. PCOS is regarded as a disease process that not only greatly reduces a woman’s chances of conceiving, but also increases her risk for developing type 2 diabetes mellitus, cardiovascular disease, and endometrial cancer.1 Fortunately, there are various forms of treatment for PCOS, ranging from pharmaceutical drugs to supplements that, along with lifestyle modifications, have proven to be helpful in the management of the disease.
Inositol
One supplement of particular interest is inositol. Going back through history once more, German physician, Johannes Joseph Scherer, first identified inositol in muscle tissue in 1850, and named the compound using the Greek root inos, meaning sinew, and –ose, denoting sugar. The close resemblance of inositol to the chemical structure of glucose, along with its colorless, crystalline appearance, was noted at the time; however, it wasn’t until 1988 that Larner et al recognized the compound’s role in chemically mediating insulin.6
It is now known that 2 of the 9 stereoisomers of inositol – myo-inositol (MI) and D-chiro-inositol (DCI) – are found throughout the body. Larner explored the relationship between the two and suggested that individuals with type 2 diabetes mellitus have an altered MI to DCI ratio. Specifically, he found that DCI levels in these patients’ urine were depressed while their MI levels were elevated. It was proposed that the imbalance was due to a defect in the conversion of MI to DCI.6 Both forms of inositol have been shown to improve PCOS symptoms, though researchers suspect that each has its own role in the management of the condition.
Myo-inositol vs D-chiro-inositol
A March, 2014, study reported on 50 women with PCOS, who for 6 months were treated daily with either 4 g of myo-inositol plus 400 µg of folic acid, or 1 g of D-chiro-inositol plus 400 µg of folic acid.7 It was found that “both the forms of inositol were effective in improving ovarian function and metabolism in patients with PCOS, although myo-inositol showed the most marked effect on the metabolic profile, whereas D-chiro-inositol reduced hyperandrogenism better.7”
Another recent study reported outcomes of 100 women undergoing in-vitro fertilization who received either daily DCI (500 mg) or a combined MI and DCI supplement (1.1 g MI and 27.6 mg DCI). Upon completion of treatment, it was found that the women taking the MI-DCI combination experienced greater benefit than those taking DCI alone. Specifically, they produced fewer degenerated oocytes, and had a greater amount of mature oocytes, therefore a higher embryo quality and fertilization rate.8
Key features of PCOS include obesity, acne, and hirsutism; however, there are numerous ways in which PCOS can manifest. The stereotypical image of PCOS patients presenting with a high body mass index (BMI), hirsutism, and hyperinsulinemia is no longer the rule. In fact, reports suggest only about half of women with PCOS are overweight or obese; the other half have a normal body mass – these are referred to as “lean” PCOS cases.9 The other classic symptom, hyperinsulinemia, may or may not be present in the disorder. Several studies over the last few years have taken these variations into account. Most have found that regardless of type (lean, obese, insulin-resistant, or non-insulin-resistant), the incorporation of myo-inositol into a treatment plan for PCOS is beneficial.
In a study involving 42 overweight women with BMIs greater than 25.5, improvements due to myo-inositol (2 g/day) and folic acid (200 µg/d) were found to be more significant in the group that had baseline fasting insulin levels greater than 12 µU/mL. However, the women who had insulin levels less than 12 µU/mL still benefited in terms of endocrine parameters and insulin sensitivity.10 Similarly, hormonal parameters improved in 24 women of normal weight and no presence of hyperinsulinemia who received a 12-week combination of myo-inositol (1500 mg), lactoferrin (100 mg), and bromelain (20 mg) BID, although there was no change in BMI.11
Myo-inositol vs Metformin
When compared to conventional treatment using metformin, myo-inositol proves to be just as effective, if not more effective, in treating PCOS symptoms.
In 2010, Raffone and colleagues reported the results of a trial in which 42 women with PCOS were randomized in double-blind fashion to receive either 1500 mg of metformin per day or 4 g of myo-inositol in combination with 400 µg of folic acid.12 Spontaneous ovulation was achieved in 65% of the patients receiving MI, with 30% achieving pregnancy. In comparison, of the women receiving metformin, only 50% ovulated spontaneously, resulting in 18.3% becoming pregnant.12 A 2012 study compared the effect of diet alone, diet combined with metformin, or diet plus metformin and myo-inositol. Results suggested that weight loss was linked to the use of metformin, whereas menstrual cycle regulation was primarily dependent on the use of myo-inositol.13
Comments
The PCOS genotype may have offered survival advantage once upon a time; however, this is no longer the case, as the condition does more harm than good for women in the modern world. Fortunately, it appears that inositol allows individuals living with PCOS to compensate for these outdated genetic pathways and reduces the shifts in biological function brought on by the specific genes. With such rapid progression of research regarding PCOS and inositol, it is uncertain where things will stand in just a few more years. For now, though, it is safe to conclude that inositol is beneficial for women with PCOS and therefore should represent a clear and simple choice in treating these patients. Additional supplementation with folic acid is recommended, as it may result in even greater improvements in symptoms and fertility outcomes.
Preternship
Becoming a naturopathic physician requires a great deal of dedication. We need to be well educated in allopathic medicine theory and practice and, at the same time, to approach patient care relying on naturopathic principles and following a complex and somewhat esoteric hierarchy of treatment and cure. A new layer of educational competency has been added to our exiting challenges: we ask our doctors to practice what is called evidenced-based medicine (EBM). The definitions of EBM are broad, and while the gold standard of efficacy is randomized, controlled trials (RCTs), there is width to the definitions of EBM to accept the wisdom handed down from our elders and experienced colleagues. With this shift toward EBM, I find myself devoting more time to reading and evaluating published evidence in peer-reviewed medical journals. Being able to locate, interpret, and summarize the current knowledge on a particular topic has become part of our profession’s job description.
I believe we need to take this a step further. If we are to abide by that guiding principle that defines our profession – the one about a doctor’ role as teacher – our job description now requires us to both be able to research and evaluate current scientific research and to explain it to our colleagues and – more importantly – to our patients.
“Pre-terns”
Dr Bloom and I have found that students who plan to eventually go to naturopathic school make the best receptionists for our office. Their passion for our medicine, their desire to learn, and their desire to care for people far outweighs the relatively short period of employment; they end up leaving just when we’ve come to depend on them. Over the last 2-dozen years, we have said goodbye and good luck at naturopathic school to 7 of our receptionists who are now either naturopathic doctors or on their way to graduation: http://denvernaturopathic.com/Receptionistpage.htm
You all know what an intern is, and the naturopathic variant, extern. Our receptionists go through a 1 to 2 year period as “preterns,” our own version of a pre-naturopathic school education.
Thus, our current receptionist, Megan Chmelik, was given something of a quid pro quo when she mentioned that she was hoping for a letter of reference to go with her school applications. I wanted her to learn how to research, review, and organize, and then write a paper on a topic relevant to naturopathic practice. What you see in the accompanying article is the result of that negotiation.
One would think that learning to do this would be a skill that each and every naturopathic doctor has and exercises. If our profession is to move forward, this is something all of us need to learn and be good at. I would offer to help you learn to do this, but I’ve got those 7 former employees whom I feel obligated to train first.
 Jacob Schor, ND, FABNO, is a 1991 graduate of NCNM and has practiced in Denver for the past 17 years. He served as president of the CANP from 1992 to 1999. He has served on the board of directors of the OncANP since 2006 and currently acts as secretary to the board. He is a Fellow of the ABNO. He was utterly shocked and humbled at the 2008 convention of the AANP to be presented with the Vis Award, an honor bestowed in the memory of William Mitchell. He is incredibly lucky to practice with his wife, Rena Bloom, ND. Dr Schor writes newsletters for his patients that are popular with doctors and students.
Jacob Schor, ND, FABNO, is a 1991 graduate of NCNM and has practiced in Denver for the past 17 years. He served as president of the CANP from 1992 to 1999. He has served on the board of directors of the OncANP since 2006 and currently acts as secretary to the board. He is a Fellow of the ABNO. He was utterly shocked and humbled at the 2008 convention of the AANP to be presented with the Vis Award, an honor bestowed in the memory of William Mitchell. He is incredibly lucky to practice with his wife, Rena Bloom, ND. Dr Schor writes newsletters for his patients that are popular with doctors and students.
Megan Chmelik, a former professional dancer with Ballet Arizona, is currently in her final year at Metropolitan State University of Denver. She will graduate in May of 2015 with an undergraduate degree in Integrative Therapeutic Practices, an educational program designed to prepare students for advanced studies in complementary medicine, in particular naturopathic medical school. She currently also works as a receptionist for Rena Bloom, ND, and Jacob Schor, ND, FABNO, at the Denver Naturopathic Clinic. As part of their tradition of mentoring receptionists and preparing them for naturopathic school, Dr Schor had the naive thought that Megan had adequate free time in which to both learn how to use PubMed and start writing review articles for journals such as NDNR.
References
- Tieken A, Lonnemann E. Polycystic ovarian syndrome. Physiopedia Web site. http://www.physio-pedia.com/Polycystic_Ovarian_Syndrome. Accessed September 15, 2014.
- Hanson AE. Hippocrates: Diseases of Women 1. Signs (Chic).1975;1:567-584.
- Rosner F, Munter S. The Medical Aphorism of Moses Maimonides, Volume II. New York, NY: Yeshiva University Press; 1971.
- Robinson S, Chan SP, Spacey S, et al. Postprandial thermogenesis is reduced in polycystic ovary syndrome and is associated with increased insulin resistance. Clin Endocrinol (Oxf). 1992;36(6):537-543.
- Azziz R, Dumesic D, Godarzi M. Polycystic Ovary Syndrome: An Ancient Disorder? Fertil Steril. 2011;95(5):1544-1548.
- Bizzarri M, Carlomagno G. Inositol: history of an effective therapy for Polycystic Ovary Syndrome. Eur Rev Med Pharmacol Sci. 2014;18(13):1896-1903.
- Pizzo A, Laganà AS, Barbaro L. Comparison between effects of myo-inositol and D-chiro-inositol on ovarian function and metabolic factors in women with PCOS. Gynecol Endocrinol. 2014;30(3):205-208.
- Colazingari S, Treglia M, Najjar R, Bevilacqua A. The combined therapy myo-inositol plus D-chiro-inositol, rather than D-chiro-inositol, is able to improve IVF outcomes: results from a randomized controlled trial. Arch Gynecol Obstet. 2013;288(6):1405-1411.
- Faloia E, Canibus P, Gatti C, et al. Body composition, fat distribution and metabolic characteristics in lean and obese women with polycystic ovary syndrome. J Endocrinol Invest. 2004;27(5):424-429.
- Tais S. Myo-Inositol in Polycystic Ovarian Syndrome: Supplement acts as a natural insulin sensitizer in PCOS patients. Nat Med J. Aug 2013;5(8).
- J Genazzani AD, Santagni S, Ricchieri F, et al. Myo-inositol modulates insulin and luteinizing hormone secretion in normal weight patients with polycystic ovary syndrome. Obstet Gynaecol Res. 2014;40(5):1353-1360.
- Raffone E, Rizzo P, Benedetto V. Insulin sensitiser agents alone and in co-treatment with r-FSH for ovulation induction in PCOS women. Gynecol Endocrinol. 2010;26(4):275-80.
- Le Donne M, Alibrandi A, Giarrusso R, et al. [Diet, metformin and inositol in overweight and obese women with polycystic ovary syndrome: effects on body composition]. [Article in Italian] Minerva Ginecol. 2012;64(1):23-29.







{kind=link}