
Dr. Nora Pope ND, FCP
A clinical exploration of how collaborative ND–NP care can bridge prescribing limitations, integrate restorative fertility strategies, and expand access to individualized reproductive treatment.
This article examines the clinical value of collaboration between naturopathic doctors and nurse practitioners in fertility care, particularly where prescribing limitations restrict access to pharmaceutical interventions. It explores how integrative partnerships may expand treatment options for ovulation support, hormonal optimization, and restorative reproductive care while maintaining a whole-person, root-cause approach.
This article examines the clinical and professional benefits of collaborative care between Naturopathic Doctors (NDs) and Nurse Practitioners (NPs), with a focus on expanding patient access to pharmaceutical fertility treatments. In many jurisdictions, NDs face limitations in their prescribing authority for repurposed drugs used as off-label fertility medications. By working alongside NPs, who typically hold broader prescribing privileges, NDs can ensure their patients receive comprehensive, restorative fertility care that integrates pharmaceutical support with naturopathic principles.
Introduction
In my years as a Naturopathic Doctor in Toronto from 2002 to 2019, I worked with many healthcare professionals who had a wider scope of prescribing privileges. In the sub-specialty of infertility, progesterone was the primary medication I could access through collaborating with other providers. As greater understanding to the root causes of infertility come to light, an increasing number of drug classes are revealing whole-body benefits for patients. Since many off-label drugs are out of reach for NDs, Nurse Practitioners can fill this gap, especially if they have the following credentials:
- WHNP (Women’s Health Nurse Practitioner) specialize in comprehensive lifelong healthcare for women. Like NDs, they can communicate a diagnosis, order tests and prescribe medication. Under gynecological care, they conduct annual pelvic exams, Pap smears and breast cancer screenings. In reproductive health, they treat menstrual disorders and infertility. In Obstetric care, they provide prenatal and postpartum care.
- APRN (Advanced Practice Registered Nurse) is a highly trained healthcare professional who has a master’s or doctoral degree in nursing. They have an expanded scope of practice allowing them to examine, diagnose, order tests and prescribe medication. APRN is an umbrella term which covers NPs.
- Jurisdictional Prescribing Authority for Fertility Medications
Many naturopathic jurisdictions across North America are seeking increased scope of practice in the pharmacological sphere. Low-dose medications are philosophically consistent with naturopathic philosophy and are a welcome addition to the scope of practice. In the meantime, working with a nurse practitioner can help NDs access newer and broader fertility treatments.
Lower dosing fits into a larger trend of repurposing existing drugs for off-label uses. As scientific advancements shed light on how these drugs affect human reproduction, the future of fertility treatment looks increasingly innovative.
The following table outlines the prescribing landscape for the fertility-related drugs discussed in this article, comparing the authority of NDs and NPs across North American jurisdictions. Some of these medications fall under a “low-dose” category.
Below are some examples of established and off-label medications available in the scope of trained NPs:
| Medication | ND Prescribing Authority | NP Prescribing Authority |
|---|---|---|
| Bio-identical Progesterone & Estrogen | Allowed in regulated provinces (e.g., ON, BC) and US states (e.g., AZ, OR, WA) with prescribing certification. | Broadly allowed across North America in almost all jurisdictions. |
| hCG (Human Chorionic Gonadotropin) | Restricted in many jurisdictions; often requires specific hormonal prescribing rights or is outside scope for NDs. | Allowed as part of primary or specialized care in most US states and Canadian provinces. |
| Low Dose Naltrexone (LDN) | Scope varies; often allowed in jurisdictions with “Full” or “Primary Care” prescribing rights (e.g., OR, WA, BC). | Allowed; commonly used off label by NPs in integrative and functional medicine. |
| Letrozole / Low Dose Clomiphene | Restricted; often considered “specialist” fertility drugs outside the standard ND formulary in most regions. | Broadly allowed; NPs can prescribe these for ovulation induction in most jurisdictions. |
| Low Dose Antibiotics (e.g., Doxycycline for endometritis) | Restricted in many ND jurisdictions to specific lists (e.g., URIs or UTIs), often excluding obstetric/fertility specific uses. | Full prescribing authority for antibiotics across North America. |
| Oral Dexamethasone | Restricted for NDs; often limited to topical use or specific emergency protocols in limited states. | Broadly allowed; used by NPs for a variety of inflammatory and endocrine conditions. |
- Benefits of Pharmaceutical Integration in Naturopathic Fertility Care
The integration of specific pharmaceutical agents into a naturopathic fertility protocol offers a synergistic approach to “Restorative Fertility”. While some NDs excel at cycle charting and lifestyle interventions, the addition of targeted medications can overcome physiological barriers that may not respond to natural therapies alone.
Hormonal Support: Progesterone
Bio-identical progesterone is a cornerstone of restorative fertility, particularly for patients with Luteal Phase Deficiency (LPD). Naturopathic monitoring through cycle charting allows for precise timing—administering progesterone from “Peak +3” to “Peak +12” to mimic the body’s natural rhythm during the Post Peak phase. See my article “Day 21 No More” for a detailed explanation of synching up the patient’s dosing with her menstrual chart.
Progesterone supports implantation by stabilizing the uterine lining, inhibiting myometrial contractions, and promoting an immunomodulatory environment that protects the conceptus from rejection.
The tables below demonstrate the rationale for dosing on “Peak +3 to Peak +12”
The chart below is an example of the classic 28-day cycle:

28-day Cycle Chart: 14 days before and after the Peak Day. Cycle Day 21 is the mid-luteal day. Dosing progesterone on Peak +3 to Peak +12 corresponds to CD 17 to CD 26.
The chart below shows three healthy cycles of varying length: 28, 24 and 33 days.
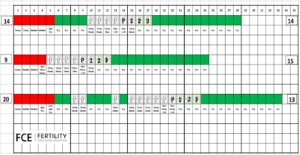
Mid-luteal day is Peak +7. Top chart that falls on CD 21. Middle chart is CD 16. Bottom chart is CD 27. Peak +3 to Peak +12 days are: Top chart – CD 17 to 26; middle chart – CD 12 to 21; bottom chart – CD 23 to 32
Prometrium, the pharmaceutical form of bio-identical progesterone only comes in 100mg or 200 mg capsules. They can be ingested orally or inserted vaginally. Should your patient require a higher dose, compounding pharmacies can tailor the dosage. In some cases, some patients may require up to 1000mg a day.
Ovulation Induction and Ovarian Function
For patients with Polyendocrine Metabolic Ovarian Syndrome (PMOS) or anovulation, medications like Letrozole and Clomiphene are standard of care. Letrozole, an aromatase inhibitor, blocks estrogen production to trigger a natural rise in Follicle Stimulating Hormone (FSH), making follicles more sensitive and aiding ovulation. Naturopathic doctors can enhance this effect by co-prescribing botanicals like green tea or indole-3 carbinol to manage overall estrogen metabolism.
Similarly, Human Chorionic Gonadotropin (hCG) can be used off label to stimulate the corpus luteum or induce ovulation when a follicle reaches maturity (typically 1.8cm on ultrasound; ideally up to 2.2cm). This pharmaceutical intervention is particularly potent when paired with naturopathic supports like Vitex, which further modulates the LH/FSH ratio.
Novel Applications: Low Dose Naltrexone and dexamethasone
Low Dose Naltrexone (LDN) represents another advancement in treating infertility associated with endorphin deficiencies and autoimmune factors. LDN works by causing a brief opioid blockade that triggers an adaptive increase in endorphins, which in turn improves immunomodulation and may improve egg quality (AMH) and uterine receptivity.
Dexamethasone, while a potent steroid, is used at very low doses (0.25 mg qhs) to treat idiopathic hyperandrogenism. By suppressing overactive adrenal output, it can restore ovulation in “lean variant” PMOS patients who do not respond to standard treatments like Metformin. Dexamethasone is used to address “dry cycles” or low follicular-phase levels of estrogen that inhibit ovulation.
Conclusion
Many naturopathic jurisdictions across North America are seeking increased scope of practice in the pharmacological sphere. Low-dose medications are philosophically consistent with naturopathic philosophy and are a welcome addition to the scope of practice.
By collaborating with Nurse Practitioners, Naturopathic Doctors can bridge the gap between holistic monitoring and advanced medical intervention. This partnership allows for a “best of both worlds” approach: the meticulous cycle tracking and root-cause analysis of naturopathy, combined with the powerful, targeted pharmaceutical tools necessary to achieve and maintain a healthy pregnancy.
Bio:
 Nora Jane Pope, ND, FCP, creates, produces and hosts Continuing Medical Education programs. She is a graduate of McGill University and the Canadian College of Naturopathic Medicine. She was a naturopathic doctor and Creighton Model FertilityCare™ Practitioner in Toronto from 2002-2019.
Nora Jane Pope, ND, FCP, creates, produces and hosts Continuing Medical Education programs. She is a graduate of McGill University and the Canadian College of Naturopathic Medicine. She was a naturopathic doctor and Creighton Model FertilityCare™ Practitioner in Toronto from 2002-2019.
Since 1994, Pope has been a user and advocate of Fertility Awareness and Cycle Charting and integrated these into her practice. She completed advanced training in Obstetrics and Gynaecology in NaProTechnology and has published articles on fertility in NDNR, the OAND Journal and Midwifery Today.
Pope is a member of the American Academy of FertilityCare Professionals and the International Institute of Restorative Reproductive Medicine. She has a special interest in Bio-identical progesterone, off-label prescribing, and harnessing drug-herb interactions to improve outcomes. In 2020, she co-founded Fertility Continuing Education to deliver accredited CME programs to healthcare professionals around the world. To view which Obstetrics and Pharmacology credits are available to NDs, Visit her website












