
Mary Fu, BA, MA
Jennifer Brusewitz, ND
Student Scholarship – Honorable Mention Case Study
The Therapeutic Order describes the foundational philosophical principles of naturopathic medicine and serves as a guiding force in its modern practice (Figure 1).1 The following case illustrates the use of topical castor oil, within the context of the Therapeutic Order, for age-related cataract in a 68-year-old male. This patient, like so many of our patients, came to us already engaged with ongoing higher-order interventions. His case is notable, however, in that he is dependent on them for organ function. In spite of this, he is determined to work within the foundational layers of the Therapeutic Order to improve his vision and overall health.
Figure 1. Therapeutic Order Pyramid
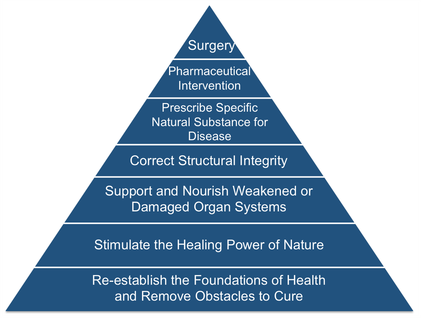
(Adapted from Zeff J, et al; 2006)1
The Patient
Our patient is a 68-year-old quadriplegic male who first presented to our clinic seeking treatment for cataract of the right eye, a diagnosis that was made by his ophthalmologist 5 years prior. He reported a notable decline in vision after a 7-month period of hospitalization following a surgical complication. Subsequently, he experienced progressive difficulty seeing computer screens and reading books, due to decreased visual acuity and increasing sensitivity to light. At the time of presentation, he had already been prescribed multiple pairs of glasses to correct his vision, without success.
His past medical history was significant for a number of cardiovascular and pulmonary events associated with paralysis. Without adequate blood- and lymphatic circulation to deliver nutrients and oxygen, the small vessels of the kidneys and eyes are the first to be impacted. Furthermore, he was being managed on multiple medications that help maintain organ function but which also have adverse effects, particularly on eye health. These medications included alendronate (photosensitivity, uveitis), pregabalin (blurry vision), baclofen (amblyopia), and amiodarone (visual disturbances, photosensitivity). The effects of long-term amiodarone use on eye health are perhaps the most well-researched and include decreased visual acuity due to optic neuropathy, optic disc edema, and corneal deposits, which in some cases also cause visions of halos around lights, photophobia, dry eyes, and blurred vision.2
The visual exam at his initial visit revealed OD 20/100, OS 20/50, OU 20/50. The red reflex was present bilaterally, indicating a mild presentation of cataract, and the direct and consensual pupillary reflexes were diminished.
Age-Related Cataract
Cataract is the leading cause of blindness in the world, accounting for half of all cases.3 The 10-year incidence of cataract is estimated to be 54% for a US population aged 43 to 86 years.4
Age-related cataract development is painless, and the decline in vision is progressive. The lens is composed of stratified epithelial cells that are arranged in an ordered but highly complex structure. It is rich in cytoplasmic crystalline proteins, which impart transparency to the lens. Unlike other epithelia, the lens does not shed its nonviable cells and is more susceptible to the degenerative effects of aging and photo-oxidative damage.5 Most risk factors are environmental and lifestyle stressors that increase toxic burden and deplete the body’s natural antioxidants, including age, smoking, alcohol consumption, excessive sunlight exposure, poor lifestyle habits such as malnutrition and physical inactivity, metabolic syndrome and diabetes mellitus, lead exposure, ocular trauma and infections, and the use of drugs such as systemic corticosteroids and statins.6 Among these, our patient’s most significant risk factors included his advancing age, physical inactivity, organ compromise, and use of pharmaceutical drugs that adversely affect vision and eye health.
Currently, the standard treatment of cataract is intraocular lens implantation to restore normal vision.7 This surgical procedure is usually pursued when the diminishing visual acuity can no longer be corrected by spectacles and begins to significantly affect activities of daily living (ADLs).8
Castor Oil & Eye Health
Castor oil, which is extracted and processed from the castor bean Ricinus communis, is a traditional remedy whose therapeutic use dates back to at least 1550 BC. It was first described as being used in the form of eye drops to protect the eyes from irritation.9 Among its healing properties, castor oil is notable for its ability to quell inflammation and promote lymphatic circulation. It has been used both externally and internally for a wide variety of conditions, from joint inflammation to uterine fibroids. The use of castor oil, especially as the heated compress we know today, was popularized by the work of Edgar Cayce (1877-1945), an American mystic who was also dubbed the “father of holistic medicine.”10
In recent years, studies on the use of castor oil for eyes have found that it aids in the reformation of the lipid layer of the tear film and prevents evaporation of the existing tear film.11 It also increases the lubrication ability of eye drops and improves meibomian gland function in patients with gland dysfunction.12 Several commercial eye drops today include castor oil as one of their active ingredients. It is well established that a healthy tear film is important for supplying nutrients and oxygen to the eye, preventing infection, and optimizing vision.13 We took advantage of these medicinal properties of castor oil in a topical application for our patient with mild cataract.
Treatments Based on the Therapeutic Order
We initiated several types of intervention at our patient’s first office visit, working primarily within the bottom 3 tiers of the Therapeutic Order. These included nutrition, castor oil, and homeopathic remedies (Figure 1).
The first step of the Therapeutic Order is to remove obstacles to health, which most commonly include poor diet and sleep, sedentary habits, excessive stress, inadequate social support, and spiritual disharmony. As previously discussed, the patient presented with several obstacles to cure, most notably paralysis and dependence on pharmaceutical medications. However, he already had established many elements of the foundational layer of the Therapeutic Order. He boasted of a robust social support network comprised of family, caretakers, and long-time childhood friends. He was also mindful of getting daily sunshine and fresh air despite his physical limitations, and he had few sleep complaints. Furthermore, he came to us already eating a nutritious, plant-based diet of fruits and vegetables, healthy fats, and proteins. We built on this foundation by recommending that he increase his intake of berries and tomatoes, which are high in several key nutrients found to be essential for eye function, including lutein, zeaxanthin, and antioxidants such as vitamin C. According to a 2008 study, diets rich in lutein and zeaxanthin were moderately associated with decreased prevalence of nuclear cataract in older women.14 Similarly, vitamin C, in doses of at least 1000 mg daily, was found to result in a significant slowing of cataract progression, with only a handful of patients requiring surgery over the 11-year study period.15
We then moved up the pyramid to stimulate the body’s innate healing mechanisms. This is usually accomplished through a variety of gentle therapies that promote whole-body healing, such as hydrotherapy, homeopathy, acupuncture, and meditation. In this case, we employed the use of castor oil for its emollient properties and ability to promote circulation. We recommended applying 1 drop of castor oil to the inner canthus of each eye nightly at bedtime, with the goal of allowing the oil to work overnight without the temporary side effect of blurred vision. Concurrent support included contrast hydrotherapy in the form of alternating warm and cool compresses to the eyes, which helps increase blood flow and further improve nutrient delivery and waste removal.
At times it may be necessary to support organ systems that have become weakened or damaged from longstanding disease and suppressed vitality. Botanical medicine, specific nutrient prescriptions, as well as previously mentioned modalities such homeopathic remedies, are among the many targeted therapies available. We used low-potency, combination homeopathics that address specific organ systems of elimination. They work synergistically with other therapies to ensure that the patient can discharge accumulated toxins through 1 of 4 primary emunctories: skin, intestines, lungs, and the urinary system. We focused primarily on supporting the liver’s function as the seat of elimination and the sorting of waste by using remedies that work at the cellular level to relieve hepatic congestion. We also supported the patient’s kidney function in its vital role in blood filtration.
In addition to homeopathic remedies, the patient began taking the supplementary nutrients lutein and zeaxanthin, which complemented dietary intake to help protect against oxidative damage. He also started taking Gingko biloba and Vaccinium myrtillus (bilberry), both of which have been found to improve visual function and retinal blood flow in patients with normal-tension glaucoma.16
Support to be considered in the future included Cineraria maritima and N-acetylcarnosine (NAC) eye drops. Cineraria maritima is a perennial plant of the Asteraceae family, native to the Mediterranean.17 Extracts of the plant in the form of eye drops have been studied for the treatment of cataracts as early as the beginning of the 20th century. Its healing effects are attributed to its potassium and iodine content, thought to be important for lens health.18 NAC, when applied to the surface of the eye, is metabolized into the protein L-carnosine, which has an antioxidant effect on the lens and has been shown to improve visual acuity and reduce glare sensitivity in patients with cataracts.19,20 The patient would also need to be monitored for increased risk of glaucoma, secondary to cataract formation, which could warrant earlier surgical intervention.
Outcomes & Conclusion
At the 1-month follow-up visit, the patient reported adherence to the recommended therapies with no difficulties, except that he took it upon himself to increase the castor oil drops to twice daily with no adverse effects. He reported subjective improvement in visual acuity. Visual exam revealed that while the left eye remained stable at 20/50, visual acuity in his affected right eye had improved from 20/100 (1 month earlier) to 20/70. At the 3-month follow-up, visual acuity remained stable, and the patient again reported continued subjective improvement in vision, stating that he was better able to see the clock on his ventilator.
Our patient came to us with a commitment to adhering to the recommended treatment plan for at least 1 year, and he understood the importance of consistency. At the 1 and 3-month follow-up visits, he was happy to discover that his visual acuity had already improved. His case demonstrates that despite significant obstacles to cure, the body nevertheless reveals its miraculous ability to heal when working simply and diligently on the foundational layers of health through the Therapeutic Order.
References:
- Zeff J, Snider P, Myers SP. A Hierarchy of Healing: The Therapeutic Order. In: Pizzorno J, Murray MT, eds. Textbook of Natural Medicine, Volume 1. 3rd ed. St Louis, MI: Churchill Livingstone Elsevier; 2006: 27-39.
- Erdurmus M, Selcoki Y, Yagci R, Hepsen IF. Amiodarone-induced keratopathy: full-thickness corneal involvement. Eye Contact Lens. 2008;34(2):131-132.
- Thylefors B, Négrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness. Bull World Health Organ. 1995;73(1):115-121.
- Klein BE, Klein R, Lee KE. Incidence of age-related cataract over a 10-year interval: the Beaver Dam Eye Study. Ophthalmology. 2002;109(11):2052-2057.
- Kuszak JR, Deutsch TA, Brown HG. Anatomy of aged and senile cataractous lens. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. Philadelphia, PA: WB Saunders Company; 1994: 564.
- West SK, Valmadrid CT. Epidemiology of risk factors for age-related cataract. Surv Ophthalmol. 1995;39(4):323-334.
- Asbell PA, Dualan I, Mindel J, et al. Age-related cataract. Lancet. 2005;365(9459):599-609.
- Jacobs D. Cataract in Adult. 2017. In: Post T, ed. UpToDate. Waltham, MA. Available at: https://www.uptodate.com. Accessed August 24, 2017.
- Gaddum JH. Pharmacology. 3rd ed. New York, NY: Oxford University Press; 1949.
- McGarey WA. The Oil That Heals: A Physician’s Successes with Castor Oil Treatments. Virginia Beach, Virginia: A.R.E. Press; 1993.
- Di Pascuale MA, Goto E, Tseng SC. Sequential changes of lipid tear film after the instillation of a single drop of a new emulsion eye drop in dry eye patients. Ophthalmology. 2004;111(4):783-791.
- Goto E, Shimazaki J, Monden J, et al. Low-concentration homogenized castor oil eye drops for noninflamed obstructive meibomian gland dysfunction. Ophthalmology. 2002;109(11):2030-2035.
- Montés-Micó R. Role of the tear film in the optical quality of the human eye. J Cataract Refract Surg.2007;33(9):1631-1635.
- Moeller SM, Voland R, Tinker L, et al. Associations between age-related nuclear cataract and lutein and zeaxanthin in the diet and serum in the Carotenoids in the Age-Related Eye Disease Study, an Ancillary Study of the Women’s Health Initiative. Arch Ophthalmol. 2008;126(3):354-364.
- Bouton S. Vitamin C and the aging eye. Arch Intern Med. 1939;63:930-945.
- Shim SH, Kim JM, Choi CY, et al. Ginkgo biloba extract and bilberry anthocyanins improve visual function in patients with normal tension glaucoma. J Med Food. 2012;15(9):818-823.
- Cineraria Maritima. A Modern Herbal, by Mrs. M. Grieve. Botanical.com Web site. http://www.botanical.com/botanical/mgmh/c/cinmar68.html#des. Accessed September 14, 2017.
- Burdon-Cooper J. Cineraria maritima and the treatment of cataract. Br Med J. 1936;1(3914):85.
- Dubois VD, Bastawrous A. N-acetylcarnosine (NAC) drops for age-related cataract. Cochrane Database Syst Rev. 2017;28(2):CD009493.
- Babzizhayev MA, Deyev AI, Yermakova VN, et al. Efficacy of N-acetylcarnosine in the treatment of cataracts. Drugs R D. 2002;3(2):87-103.
Image Copyright: <a href=’https://www.123rf.com/profile_bdspn’>bdspn / 123RF Stock Photo</a>
 Mary Fu, BA, MA, is a naturopathic medical student in her last year at the National University of Natural Medicine, in Portland, OR. Mary has a background in psychology and social science research from UCLA and the RAND Corporation. In her future clinical practice, she hopes to serve populations with poor access to healthcare.
Mary Fu, BA, MA, is a naturopathic medical student in her last year at the National University of Natural Medicine, in Portland, OR. Mary has a background in psychology and social science research from UCLA and the RAND Corporation. In her future clinical practice, she hopes to serve populations with poor access to healthcare.
***
 Jennifer Brusewitz, ND, is a 2000 graduate of the National University of Naturopathic Medicine (NUNM), in Portland, OR. She is academic faculty in the MScN and MSOM programs at NUNM, and clinical faculty at NUNM’s teaching clinics.
Jennifer Brusewitz, ND, is a 2000 graduate of the National University of Naturopathic Medicine (NUNM), in Portland, OR. She is academic faculty in the MScN and MSOM programs at NUNM, and clinical faculty at NUNM’s teaching clinics.















