
")
A preventive cardiology case demonstrates how advanced imaging, aggressive lipid optimization, and integrative therapies can reduce coronary plaque burden in a high-risk patient.
Dr. Stephen Parcell, ND
This case report examines the regression of coronary artery plaque in a high-risk patient using AI-driven coronary CT angiography, advanced lipid testing, and an integrative cardiovascular treatment strategy. The findings underscore the value of early detection, aggressive lipid optimization, and combined natural and prescription interventions in reducing atherosclerotic burden and cardiovascular risk.
Abstract
Background: Subclinical atherosclerosis may not be detected by conventional cardiovascular screening, particularly in individuals with mixed dyslipidemia and a significant family history of cardiovascular disease. Advanced imaging and biomarker analysis can enhance early risk identification and preventive management.
Case Presentation: A 66-year-old female with a strong familial history of cardiovascular disease presented for preventive cardiology evaluation due to abnormal lipid markers and concerns regarding arterial health. Her medical history included untreated hypothyroidism, hyperlipidemia, hypertension, vitamin D deficiency, and hormone replacement. Advanced lipid testing demonstrated elevated LDL particle number, apolipoprotein B, triglycerides, and PLA2, consistent with increased atherogenic and inflammatory risk. Coronary CT angiography with AI-assisted plaque analysis revealed a 38% stenosis of the proximal left anterior descending artery with mixed plaque morphology, including rupture-prone low-density noncalcified plaque, consistent with stage 1 atherosclerosis. Carotid intima-media thickness testing demonstrated markedly accelerated vascular aging, corresponding to a vascular age of 93 years (89th percentile).
Interventions and Outcomes: A comprehensive preventive cardiology strategy was implemented, emphasizing a Mediterranean-style diet, increased aerobic exercise, treatment of hypothyroidism, and targeted nutraceutical and prescription interventions to reduce lipids and plaque. Follow-up testing showed effective treatment of hypothyroidism and a large reduction of atherogenic lipids. Repeat coronary CT angiography demonstrated a reduction in plaque volume, non-calcified plaque, and stenosis.
Conclusion: By targeting causative risk factors and optimizing lipid markers using a combination of natural and prescription treatments, lipids greatly improved and plaque decreased. This case also highlights the limitations of conventional cardiovascular screening and demonstrates the value of advanced imaging and biomarker assessment in detecting early atherosclerosis and guiding personalized preventive interventions in high-risk individuals.
Introduction
Atherosclerotic cardiovascular disease (ASCD) is a major cause of morbidity and mortality worldwide. Early diagnosis and treatment are critical for the prevention of major adverse cardiovascular events (MACE). Classic obstructive symptoms such as angina indicate advanced disease. Often, the first symptom can be Acute Coronary Syndrome (ACS). High-risk patients may be asymptomatic. Because of this, early detection using imaging and blood work is important. Diet, exercise, and nutraceuticals are evidence-based tools that can be used by the clinician to reduce cardiovascular risk in their patient population. By using imaging to assess atherosclerotic plaque burden and testing novel risk factors, better risk stratification can be achieved, especially in an intermediate risk patient.
Case Presentation
Linda, a 66-year-old female, visited in 2022, for her initial consultation. She reported a family history of heart issues on her father’s side and expressed concerns about her left carotid artery scan, LDL, and triglyceride levels, which were not favorable. Linda sought guidance on reversing the damage to her carotid artery and requested recommendations for future testing to better understand her arterial health. She was prepared to provide a blood pressure log for at least a week, as she believed blood pressure management would be a key factor in addressing her concerns.
Linda’s health goals included reversing any possible arterial damage, identifying and taking the right supplements, and learning how to prevent heart issues to avoid potential congestive heart failure in the future.
Her medical history included asthma, high blood pressure, high cholesterol, high triglycerides, Coronary artery calcium volume of 5, low thyroid, COVID-19, hives, ovarian cysts, endometriosis, severe Vitamin D deficiency, fibrocystic breast disease, and cessation of periods. She had undergone surgeries such as tonsillectomy, D&C for heavy periods, and hemorrhoid surgery.
Linda’s family medical history revealed significant cardiovascular conditions, including myocardial infarction, CHF, cholesterol issues, hypertension, and stroke. There was also a history of diabetes, osteoporosis, and Alzheimer’s disease in her family.
Diagnostic Testing:
A coronary CT angiogram (CCTA) was ordered with AI driven plaque analysis. Results revealed a 38% stenosis in the proximal LAD. All the other arteries and branches were clear. There were three types of plaque morphology noted with corresponding plaque volume: rupture-prone low-density noncalcified plaque 1.4mm3, noncalcified plaque 43.2 mm3, and calcified plaque at 7.7 mm3. This put her at plaque stage 1, with zero being the best and three being the worst according to plaque staging criteria.1
A comprehensive lipid panel with inflammation markers was ordered in addition to CBC, CMP, TSH, Ft3, Ft4, vitamin D, A1c, and iodine.
- High atherogenic particle burden: ApoB 122 mg/dL (high) and LDL particle number 2187 nmol/L (high) indicate increased cardiovascular risk.
- Unfavorable LDL profile: Pattern B with elevated small LDL (587) and medium LDL (501) and reduced LDL peak size (213.3 Å)—a high-risk, small dense LDL phenotype.
- Elevated cholesterol: Total cholesterol 247 mg/dL, LDL-C 162 mg/dL, and non-HDL-C 192 mg/dL, all above recommended targets.
- Triglycerides mildly elevated: 153 mg/dL. Optimal is <100.
- HDL mixed: HDL-C 55 mg/dL (adequate) but large HDL is low, suggesting reduced protective HDL subfractions.
- Inflammation: Lp-PLA2 mildly elevated (129), while hs-CRP is low (0.7 mg/L).
- Cholesterol ratio acceptable: Chol/HDL ratio 4.5.
- Lip (a) normal: 10 nmol/L
- Iodine low: 38 ug/L
- TSH high: 7.6: mLU/L
- Vitamin D low: 11 (nmol/L)
Despite low systemic inflammation and acceptable HDL-C, the lipid profile shows markedly elevated atherogenic particles and small dense LDL, consistent with increased ASCVD risk. An elevated Lp-PLA₂ suggests higher cardiovascular risk due to inflamed, unstable plaque, supporting more aggressive risk-factor modification even when systemic inflammation markers are low. (An elevated Lp-PLA₂ suggests higher cardiovascular risk due to inflamed, unstable plaque, supporting more aggressive risk-factor modification even when systemic inflammation markers are low).2
Interventions
The following interventions were chosen to target lipids, arterial health, hypothyroidism, and both vitamin D and iodine deficiency.
- Green tea extract – 1 cap bid:
Green tea extract (GTE), rich in catechins—especially EGCG—can modestly improve lipid profiles in humans. Mechanisms include inhibiting intestinal cholesterol absorption, increasing hepatic LDL clearance, and reducing triglyceride synthesis. Clinical studies show modest reductions in LDL-C (≈5–10 mg/dL) and total cholesterol, with minimal effects on HDL and triglycerides. Benefits are greatest in individuals with dyslipidemia and when combined with diet and lifestyle interventions.3 GTE is generally well tolerated; high doses (>800 mg/day of EGCG) may rarely affect liver enzymes.
- Tocotrienols – 300 mg bid:
Tocotrienols are vitamin E isoforms with antioxidant properties that can influence lipid metabolism. They may modestly improve lipid profiles in humans, primarily by raising HDL cholesterol and decreasing LDL cholesterol. The lipid-lowering potential is thought to result from inhibiting HMG-CoA reductase transcription, reducing cholesterol synthesis, and from antioxidant effects that protect lipoproteins from oxidative damage.4
Tocotrienols provide cardiovascular benefits beyond lipid lowering, primarily through improvements in vascular biology rather than direct effects on heart muscle mechanics. Human and mechanistic evidence supports benefits to endothelial function, arterial compliance, and vascular inflammation, likely via enhanced nitric oxide signaling and reduced oxidative stress. These effects may modestly lower blood pressure and reduce atherosclerotic progression independent of lipid changes.5
- Red yeast rice – 900 mg bid:
Red yeast rice (RYR), containing monacolin K (identical to lovastatin), has been shown in randomized trials and meta-analyses to lower total cholesterol, LDL-C, and triglycerides, with modest increases in HDL-C. Pooled data show reductions of ≈30 mg/dL LDL-C and ≈33 mg/dL total cholesterol over 8–12 weeks. Its mechanism is HMG-CoA reductase inhibition, similar to statins.6 Effects are dose-dependent, but variability in monacolin content across preparations can affect efficacy. There are human studies comparing tolerability of red yeast rice with statins that suggest red yeast rice may be better tolerated, particularly regarding muscle symptoms in statin-intolerant patients.7
- Extended-release niacin – 500 mg bid with food:
Extended-release niacin (ER niacin) has been shown in clinical studies to favorably modify the lipid profile in humans. It raises HDL cholesterol, typically by 15–25%, while also lowering LDL cholesterol, total cholesterol, and triglycerides. ER niacin can improve lipoprotein particle profiles, shifting toward larger, less atherogenic HDL and LDL particles, and may reduce apolipoprotein B, non-HDL cholesterol, and Lp(a) in some individuals. These lipid-modifying effects are attributed to niacin’s actions on fatty acid mobilization and lipoprotein synthesis pathways.8 Extended-release formulations improve tolerability by reducing flushing compared with immediate-release niacin.
Several clinical imaging and angiographic studies have investigated whether niacin can slow or reverse atherosclerotic plaque progression in humans. The HDL-Atherosclerosis Treatment Study (HATS), a randomized, placebo-controlled trial in patients with coronary heart disease and low HDL, found that the combination of simvastatin plus niacin was associated with angiographic regression of coronary stenoses and a marked reduction in clinical cardiovascular events compared with placebo or antioxidant therapy, suggesting real atheroma regression and benefit beyond LDL lowering alone. Smaller intravascular ultrasound (IVUS) studies have similarly shown that niacin combined with statin therapy reduced total and percent atheroma volume more than statin alone, with greater decreases in plaque volume and inflammatory markers. Non-invasive MRI imaging trials, such as the Oxford Niaspan Study, demonstrated that extended-release niacin added to statin therapy reduced carotid artery wall area, a surrogate for plaque burden, compared with statin alone.9
- Vitamin D+K2 – 5,000/ 400 mcg iu qd:
Vitamin D influences cardiovascular health through multiple biologically plausible pathways beyond its classical role in bone metabolism. Vitamin D receptors are expressed in vascular smooth muscle cells, endothelial cells, and cardiomyocytes, allowing vitamin D to modulate cardiovascular function at a cellular level. Mechanistically, vitamin D may suppress renin–angiotensin–aldosterone system activity, which can reduce blood pressure and vascular remodeling; enhance endothelial nitric oxide availability, improving vasodilation; and reduce inflammation and oxidative stress, which contribute to atherosclerosis and arterial stiffening. Vitamin D is also implicated in modulating immune signaling, reducing pro-inflammatory cytokines, and potentially favorably affecting dyslipidemia and insulin resistance, factors linked to cardiovascular risk. Observational studies consistently find that low serum 25-hydroxyvitamin D levels correlate with higher incidences of hypertension, atherosclerosis, heart failure, and overall cardiovascular risk, though randomized controlled trials of supplementation have produced mixed results, partly due to variability in dosing, baseline vitamin D status, and study design. A recent review highlighted these associations, described potential mechanisms linking vitamin D deficiency to cardiovascular pathology, and called for further research to clarify its role in clinical cardiovascular prevention and management.10
- Pomegranate – 400 mg qd:
Pomegranate (Punica granatum) supports cardiovascular health through multiple complementary mechanisms driven largely by its rich polyphenol content (including punicalagins, anthocyanins, and other flavonoids). These compounds exert potent antioxidant effects, protecting lipoproteins such as LDL and HDL from oxidative modification—a key early step in atherogenesis—and enhancing HDL-associated paraoxonase activity, which further reduces oxidized lipids and foam-cell formation in arterial walls. Pomegranate intake has been associated with improvements in blood pressure via enhanced endothelial function, increased nitric oxide bioavailability, and mild inhibition of angiotensin-converting enzyme activity, leading to lower systolic and diastolic pressures in some clinical studies. Anti-inflammatory actions include reductions in pro-inflammatory cytokines (e.g., IL-6 and TNF-α), which can mitigate vascular inflammation and endothelial dysfunction. Additional benefits observed in human trials and meta-analyses include favorable shifts in lipid profiles (reducing total cholesterol and raising HDL) and modest improvements in glycemic control, body mass index, and other cardiometabolic risk factors. Overall, pomegranate’s effects are pleiotropic—antioxidant, anti-inflammatory, anti-atherogenic, and vasoprotective—acting on vascular walls, lipoprotein particles, and systemic metabolic processes to support cardiovascular health.11
- Ezetimibe – 10 mg hs:
Ezetimibe lowers LDL-cholesterol by inhibiting the intestinal NPC1L1 cholesterol transporter, reducing absorption of dietary and biliary cholesterol. As monotherapy, it lowers LDL-C by ~15–20%, and when added to naturopathic treatments, provides an additional ~20–25% reduction, making it effective when statins alone are insufficient or not tolerated. Cardiovascular benefit is supported by the IMPROVE-IT trial, which showed modest but significant reductions in cardiovascular events when ezetimibe was added to statin therapy after acute coronary syndrome, consistent with incremental LDL lowering. Ezetimibe is generally well tolerated, with a safety profile similar to placebo and fewer muscle-related adverse effects than higher-dose statins, supporting its role as a safe adjunct for ASCVD risk reduction.12
- Iodine – 225 mcg qd:
This was used to treat iodine deficiency and improve thyroid function. Treating hypothyroidism can improve lipids.13
As naturopathic doctors. We should always do our best to treat the cause, educate patients about their condition and prevent morbidity, mortality and trips to the ER. It’s important to build trust with patients and make sure they understand why they’re taking what you’re giving them and doing what you’re asking them to do. By doing follow up testing more trust is built as the patient can see that the treatment is effective. This is how excellent outcomes can be achieved.
Test Don’t Guess: Coronary computed tomography angiography (CCTA) with AI-driven analysis has strong clinical validity for non-invasive assessment of coronary artery disease and risk stratification. AI-enhanced CCTA improves sensitivity and specificity for detecting stenosis and characterizing plaque while reducing observer variability and reporting time. Prospective trials have shown that AI-assisted CCTA can change clinical decision-making, increase diagnostic confidence, reduce unnecessary testing, and guide preventive therapy. Registry and multicenter data demonstrate that AI-quantified measures, such as percentage stenosis and non-calcified plaque volume, independently predict major adverse cardiovascular events, supporting both diagnostic and prognostic utility. Overall, AI-driven coronary CT analysis enhances accuracy, risk prediction, and patient management in suspected CAD.14
Treat the cause: Hyperlipidemia is a contributing factor to the development of atherosclerotic plaque. There are many factors that contribute. Naturopathic preventive cardiology should address all basic, well-understood risk factors, such as diet, stress, physical exercise, nutritional deficiencies, hypertension, endocrine conditions, environmental influences, and sleep. Even in cases where the primary treatment is based on lipid reduction, all patients should follow a healthy heart lifestyle. The dietary recommendation is a whole foods-based Mediterranean-style or similar diet. This is typically manageable for the average US citizen. Exercise prescription is variable and depends on fitness level, physical limitations, age and individual characteristics. Both strength and endurance exercise are recommended. Generally, as individuals age, more emphasis is put on strength training to maintain muscle mass and bone density. Many patients have hypertension and it’s critical to get this under control as part of a cardiovascular risk reduction program.
Outcome and Follow-Up
Aggressive therapy was decided upon after consultation with this engaged and motivated patient. In this case, the patient responded even better than expected. There are some cases where patients may not respond well to diet, lifestyle and or supplements. In other cases, diet and exercise can be enough. Sometimes natural treatment works well but lipid targets aren’t achieved, so a prescription is needed in addition. The goal is always to optimize lipid levels and achieve the best possible outcome for the patient by using whatever it takes to get there.
Image one: Lipid History
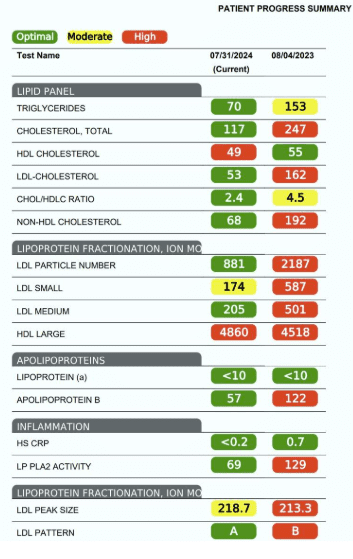
Image two: CCTA comparison
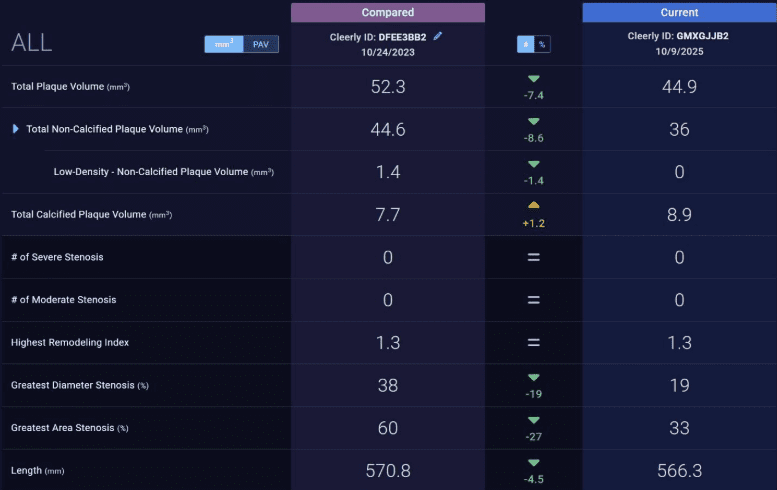
All the following decreased: Plaque volume, non-calcified plaque, area of stenosis and stenosis diameter decreased from 38% to 19%.
Discussion
This case highlights the importance of comprehensive risk assessment and biomarker analysis for clinical decision-making. This case also demonstrates that an evidence-based lipid treatment plan can be immediately effective without multiple adjustments. Most cases however, require laboratory follow-up every 3 to 6 months and ongoing adjustments to the plan, which can take up to 1 year or more. One drawback of a long, slow approach is that the growth of plaque is not addressed quickly. In this case, the patient had mainly uncalcified plaque. This type of plaque is more rupture prone and does not show up on a typical coronary calcium score. When addressing this type of plaque with an aggressive approach, plaque regression is easier to observe. This is because reverse cholesterol transport and remodeling is more likely to occur. Typically, the uncalcified plaque will turn into calcified plaque and become stable. Coronary CTA angiography is typically repeated every 2 years, and if the clinician waits too long to address risk factor treatment, it’s harder to see plaque regression within that time window.
Conclusion
In this case, the main finding was that aggressive lipid therapy, mainly using naturally derived lipid-lowering agents, was greatly effective for achieving lipid goals. Through early detection and treatment of early-stage asymptomatic atherosclerosis, angiographic plaque regression was achieved. By doing this risk of plaque rupture and obstructive stenosis is reduced.
 Dr. Stephen Parcell, ND is a licensed naturopathic physician with over two decades of clinical experience in integrative and natural medicine. A graduate of the Canadian College of Naturopathic Medicine, he blends evidence-informed naturopathic principles with a deep understanding of functional physiology to support complex chronic disease management, preventive care, and whole-person healing. Dr. Parcell has served as faculty and clinical supervisor, mentoring future clinicians in rigorous diagnostic frameworks, therapeutic nutrition, botanical medicine, endocrine and immune modulation, and lifestyle medicine. He is a frequent lecturer and contributor to professional education in naturopathic and integrative medicine, emphasizing root-cause investigation, patient empowerment, and systems-based treatment strategies that optimize long-term resilience and quality of life. He can be reached at https://www.naturemedclinic.com/steve-parcell-nd/
Dr. Stephen Parcell, ND is a licensed naturopathic physician with over two decades of clinical experience in integrative and natural medicine. A graduate of the Canadian College of Naturopathic Medicine, he blends evidence-informed naturopathic principles with a deep understanding of functional physiology to support complex chronic disease management, preventive care, and whole-person healing. Dr. Parcell has served as faculty and clinical supervisor, mentoring future clinicians in rigorous diagnostic frameworks, therapeutic nutrition, botanical medicine, endocrine and immune modulation, and lifestyle medicine. He is a frequent lecturer and contributor to professional education in naturopathic and integrative medicine, emphasizing root-cause investigation, patient empowerment, and systems-based treatment strategies that optimize long-term resilience and quality of life. He can be reached at https://www.naturemedclinic.com/steve-parcell-nd/
References:
- Coronary CTA plaque volume severity stages according to invasive coronary angiography and FFR.Min, James K. et al. Journal of Cardiovascular Computed Tomography, Volume 16, Issue 5, 415 – 422
- Corson MA, Jones PH, Davidson MH. Review of the evidence for the clinical utility of lipoprotein-associated phospholipase A2 as a cardiovascular risk marker. Am J Cardiol. 2008;101(12A):41F-50F. doi:10.1016/j.amjcard.2008.04.018
- Zamani M, Kelishadi MR, Ashtary-Larky D, et al. The effects of green tea supplementation on cardiovascular risk factors: A systematic review and meta-analysis. Front Nutr. 2023;9:1084455. Published 2023 Jan 10. doi:10.3389/fnut.2022.1084455
- Zuo S, Wang G, Han Q, et al. The effects of tocotrienol supplementation on lipid profile: A meta-analysis of randomized controlled trials. Complement Ther Med. 2020;52:102450. doi:10.1016/j.ctim.2020.102450
- Qureshi GA, et al. Tocotrienols and cardiovascular health. Review summarizing anti-oxidant, anti-inflammatory, anti-atherogenic, and experimental cardioprotective effects of tocotrienols. PubMed. PMID: 21774782.
- Li P, Wang Q, Chen K, et al. Red Yeast Rice for Hyperlipidemia: A Meta-Analysis of 15 High-Quality Randomized Controlled Trials. Front Pharmacol. 2022;12:819482. Published 2022 Jan 17. doi:10.3389/fphar.2021.819482
- Halbert et al.,Tolerability of Red Yeast Rice (2,400 mg Twice Daily) Versus Pravastatin (20 mg Twice Daily) in Patients With Previous Statin Intolerance,The American Journal of Cardiology,Volume 105, Issue 2,2010,Pages 198-204
- Ruparelia N, Digby JE, Choudhury RP. Effects of niacin on atherosclerosis and vascular function. Curr Opin Cardiol. 2011;26(1):66-70. doi:10.1097/HCO.0b013e3283410c16
- Lee JM, Robson MD, Yu LM et al. Effects of high-dose modified-release nicotinic acid on atherosclerosis and vascular function: A randomized, placebo-controlled, magnetic resonance imaging study. J Am Coll Cardiol. 2009;54:1787–1794. doi: 10.1016/j.jacc.2009.06.036.
- Agarwal P, Agarwal Y, Hameed M. Recent Advances in Association Between Vitamin D Levels and Cardiovascular Disorders. Curr Hypertens Rep. 2023 Aug;25(8):185-209. doi: 10.1007/s11906-023-01246-4. Epub 2023 May 31. PMID: 37256476.
- Mohammadi S, Heshmati J, Baziar N, et al. Impacts of supplementation with pomegranate on cardiometabolic risk factors: A systematic review and dose-response meta-analysis. Nutr Metab Cardiovasc Dis. 2025;35(10):104154. doi:10.1016/j.numecd.2025.104154
- Cannon CP, Blazing MA, Giugliano RP, et al; IMPROVE-IT Investigators. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med. 2015 Jun 18;372(25):2387-97. doi: 10.1056/NEJMoa1410489.
- Nishat S, Mueka IN, Hassan MU, et al. Effect of Levothyroxine Therapy on the Lipid Profile of Patients With Hypothyroidism: A Systematic Review. Cureus. 2024;16(7):e65218. Published 2024 Jul 23. doi:10.7759/cureus.65218
- Du M, He S, Liu J, Yuan L. Artificial Intelligence in CT Angiography for the Detection of Coronary Artery Stenosis and Calcified Plaque: A Systematic Review and Meta-analysis. Acad Radiol. 2025;32(7):3776-3787. doi:10.1016/j.acra.2025.03.054

")


















