
Dennis Godby, MA, ND
If present trends continue, 1 in 3 children born in this century in the United States will develop diabetes.1 The poorest populations in the United States suffer disproportionately from type 2 diabetes and obesity – medical conditions which are almost always preventable and reversible with targeted lifestyle management (ie, exercise, nutrition, stress reduction and attitude adjustment) and other inexpensive, mind-body solutions. This article will explore a breadth of proven and practical tools and techniques that you can implement in your practice today.
Clinical studies on obesity often use measurements of body mass index (BMI) instead of percent body fat. However, according to a Science Magazine editorial, “BMI is not an accurate measure of body fat content,” and, not surprisingly, “does not account for critical factors that contribute to health, such as where you carry your fat, proportion of muscle to fat, and sex and racial differences in body composition.2” Waist circumference is considered the best predictor of type 2 diabetes mellitus (T2D), compared to BMI, waist/hip ratio, and other anthropometric measurements.3
Changing What Can Be Changed
Common contributors to diabetes and obesity that can be changed include attitude/consciousness, unmanaged stress, poor nutrition, lack of proper exercise, hormone imbalance, intestinal permeability, environmental toxicity, neurotransmitter imbalance, and poor sleep.
The Power of Attitude
The starting point is an attitude adjustment. As Viktor Frankl said, attitude is the only thing over which we have 100% control. Every person has the capacity to be grateful, forgive, and choose health. If patients find a strong enough “WHY” to get and stay healthy, than almost any “HOW” will be manageable. One of their WHYs may be to end diabetes forever in their family, eg, for the next 7 generations.
Overcoming Stress and Anxiety
Increased abdominal obesity and binge eating is associated with increased levels of cortisol.4 Glucocorticoids increase appetite and levels of leptin, an appetite-modulating hormone.5 Increased perceived stress is associated with increased serum leptin concentrations.6 Leptin is an intricate factor in the hypothalamic-pituitary-adrenal (HPA) axis, as research shows that it is involved in the release of corticotropin-releasing hormone (CRH) in the hypothalamus, and of adrenocorticotropic hormone (ACTH) in the adrenals, and that it is regulated by glucocorticoids. Leptin and cortisol also show inverse circadian rhythms, suggestive of regulatory feedback loop.7 The hormone, ghrelin, which stimulates increased food intake and fat mass, is increased by a stress-induced rise in cortisol.8
Meditation can improve diabetes and insulin resistance. One study demonstrated a 20 mg/dL post-prandial hypoglycemic effect of a sitting, breathing meditation exercise on type 2 diabetes patients.9 The use of transcendental meditation (TM) for 16 weeks in CHD patients was also shown to improve insulin resistance and components of the metabolic syndrome.10 Laughter also confers benefits; a Japanese study showed that those who watched a brief comedy show after eating had lower glucose values than those who did not watch the program.11
Feeling “stressed” involves perception and attitude. There is no rule that says a person must perceive a particular event in a certain way. What matters most is not so much what happens to a person, but rather the emotional meaning that is attached to the event. “Unearned suffering is redemptive,” said the Reverend Martin Luther King, Jr, who knew first-hand what “unearned suffering” was all about. More accurately, MLK’s saying might be amplified to “Unearned suffering can be redemptive.” Why? Because human beings have a choice! “Superman” Christopher Reeve, with his quadriplegia, and Holocaust and concentration camp survivor, Viktor Frankl, who unjustly lost just about everything, both had a choice – to become bitter as a result of their experiences, or to accept the challenge of transforming suffering into new life. History is filled with such examples. Rather than blaming, which Wayne Dyer calls “a complete waste of time,” conflict resolution can be used.
Reducing stress and living abundantly can be accomplished by decomplicating life and living simply. I tell my patients that we must light a candle instead of cursing the darkness. Instead of focusing on deficits (lack of money, poor genetics, the past, etc), focus on what can be done. Perfectionism is a killer in my patient population and is a sure indicator of adrenal exhaustion. Perfectionism can be cured.
Reducing stress can also include lifestyle strategies such as: relaxation, meditation/prayer, guided imagery, exercise, breathing (eg, Buteyko), volunteering in the community, exercising non-judgment, striving to live in balance, and surrounding oneself with positive people who will inspire.
Nutrition and Blood Glucose Monitoring
Assume that all food and drink will raise blood sugar, unless proven otherwise through blood glucose (BG) monitoring. The most effective way to lower hemoglobin A1C is to monitor post-prandial (PP) BG 2 hours after meals, while also recording exactly what was eaten, as well as the quantity of what was eaten, for as many meals as possible. This will help to determine the patient’s best food combinations, with the goal of keeping PP BG below 140 mg/dL. (See Table 1 for recommended cutoffs.)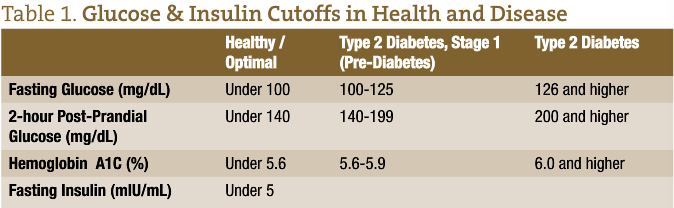
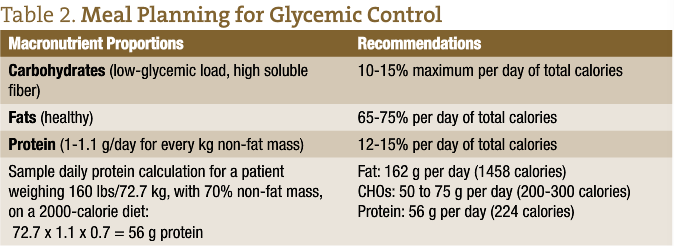
One diet to help accomplish this goal is Dr Richard Bernstein’s recommended 30 g of carbohydrates (CHOs) per day; for example, on a 2000-calories/day diet, CHOs would constitute only 6% of total calories.12 in contrast, Dr Michael Murray recommends limiting CHOs to about 10-15% of the calories, but also allows low-glycemic load and high soluble-fiber foods (peas, beans, lentils, oat bran, cherries, berries, barley, and others).13 Unlike Dr Murray, Dr Bernstein does not give much credence to soluble fiber. My own recommended protein intake is based on non-fat mass. (See Table 2 for Meal Planning recommendations.)
Since energy can only be derived from CHOs, lipids and protein, the additional calories on a CHO-restricted diet must come from fats and proteins. Since, generally speaking, CHOs raise blood sugar significantly, proteins raise it to a lesser degree, and fats raise it only negligibly, the bottom line is to always include fat, protein and soluble fiber with CHO-containing meals.
Soluble and insoluble fiber significantly improve glycemic control in patients with both T1D and T2D. Soluble fiber is more effective than insoluble fiber for reducing BG, since it attracts water like a sponge and slows down absorption of CHOs. Examples of soluble fiber include legumes (eg, lentils, peas, beans), oat bran, seeds (eg, chia, flax), almonds, fruit skins (eg, apple and pear), avocado, broccoli, carrots, and psyllium. Dose appears to make a difference; for example, 50 g of fiber per day (25 g soluble and 25 g insoluble) has been found to be more effective than 24 g (8 g soluble, 16 g insoluble) for improving glycemic control, lowering lipids, and improving insulin sensitivity.14-16 Vinegar with a meal can also reduce the 30-minute PP blood glucose response.17
Legumes, especially lentils, have a low-glycemic load. Lentils at breakfast have been found to not only produce a relatively low glucose and insulin response to the meal, but also to flatten the BG response to the subsequent lunch meal with bread.18 Resistant starch is a starch degradation product that escapes digestion in the small intestine of healthy individuals.19 Resistant starch is considered the third type of dietary fiber, as it can deliver some of the benefits of both soluble and insoluble fiber. Consumption of natural resistant starch by humans has been shown to result in a decreased glycemic response, as well as increases in insulin sensitivity, first-phase insulin secretion, and even the glycemic health of the next generation.20-32 Replacing 5.4% of the carbohydrates of a meal with resistant starch has also shown in a small study to increase fat oxidation by 23%.33
The form in which a food is consumed and the time taken to eat it also influence BG. Whole rice has less impact on BG than ground rice,34 and cooled potatoes has less impact than heated potatoes.35 According to Murray, the more processed a food, the greater the impact.13 Volunteers who ate their 2000 calories only in the morning hours lost weight, whereas eating the 2000 calories in the evening caused the same subjects to gain weight.36
Nut consumption is associated with multiple health benefits. Two large studies of women showed that nut eaters had a lower risk of type 2 diabetes.37 And in a randomized trial of 137 individuals at high risk for T2M, 4 weeks of almond consumption, with meals or as snacks, reduced PP blood glucose responses.38 In a Spanish study, 7216 adults ate a Mediterranean diet for 4.8 years; one-third of them supplemented the diet with nuts.39 Compared to non-consumers of nuts, those who ate nuts had a 39% lower mortality risk, while walnut eaters had a 45% lower risk.
Healthy fats (eg, nuts and seeds, coconut and olive oil, avocados, safe fish, organic/grass-fed/hormone-free meat, wild game) and soluble fiber increase satiety and decrease carbohydrate cravings, thereby decreasing insulin stimulation. Higher consumption of antioxidant-rich foods (such as berries and cherries) results in better control of glycemic markers.40
Advanced glycation endproducts (AGEs) are formed during high-temperature cooking. Cooking at lower temperatures and in the presence of water results in less AGE formation compared to cooking at higher temperatures and in the absence of water.19
Probiotics
According to a study published in the New England Journal of Medicine, our intestinal microbiome, along with its 5-million genes, is a powerful predictor of T2D. Among 70-year-old Scandinavian women with or without T2D, the gut microbiome “signature” was able to discriminate between these groups, as well as predict which women with impaired glucose tolerance would develop T2D.41 Probiotics can be an effective means of modifying bacterial balance in the intestine.
Artificial Sweeteners
Accumulating evidence suggests that consumption of artificially-sweetened beverages may be associated with obesity, metabolic syndrome, T2D, and cardiovascular disease, despite the lack of sugar in these products.42
Exercise
In an Amish study, men reported more physical activity than women (eg, men engaged in 10 hours per week of vigorous activity, while women engaged in 3-4 hours).43 However, levels of physical activity were high for both men and women, compared to the average North American. A total of 25% of the men and 27% of the women were overweight (BMI >25), and 0% of the men and 9% of the women were obese (BMI >30). This is significantly different than the American average, ie, one-third of Americans are obese, and over two-thirds are overweight.44
A high-intensity interval training (HIIT) session often consists of a warm-up period of exercise, followed by 3 to 10 repetitions of high-intensity exercise (at or near maximum heart rate) for 20-30 seconds, separated by medium-intensity exercise for recovery, and ending with a period of cool-down exercise. Research is suggesting that short bursts of high-intensity exercise may be the ideal form of exercise for metabolic benefits.
For example, 7 sedentary individuals were studied during 6 lower-volume, high-intensity training sessions over the course of 2 weeks. Muscle oxidative capacity and insulin sensitivity were both improved by approximately 35%.45 In a follow-up study, 1 session of HIIT (10 repetitions of 60-second cycling at 90% maximal heart rate, interspersed with 60 seconds of rest) reduced both fasting and PP blood glucose in type 2 diabetics.46 Professor Jamie Timmons believes this beneficial response is due to 80% of body’s muscles being used during HIIT, compared to 40% during gentle jogging or cycling.47
The genes that are affected by an acute bout of exercise are those that are involved in fat metabolism. Almost immediately, exercise induces genetic activation that increases production of fat-busting (lipolytic) enzymes.48 Twelve weeks of HIIT resulted in significant reductions in total abdominal, trunk, and visceral fat, as well as increases in fat-free mass and aerobic power; although in this study insulin and lipids were unaffected.49
Pumping iron can also cut the risk of T2D. A study of more than 32 000 men showed that those who lifted weights or engaged in aerobic exercise for at least 2 ½ hours per week were 34% less likely to develop T2D.50 Although weight training reduced risk independent of aerobic exercise, the combination of the two produced the greatest benefit.
Regular yoga practice may benefit health by altering leptin and adiponectin production. The hormone leptin plays key role in regulating energy intake and expenditure. It also plays a proinflammatory role, whereas adiponectin is anti-inflammatory. One study found leptin to be 36% higher among novices to yoga, compared to experts. The average adiponectin/leptin ratio in experts was nearly twice that of novices.51
Sitting kills, moving heals. Multiple, quick walks throughout the day may have an even bigger impact than a 30-minute walk before work. A study of 70 overweight or obese New Zealanders demonstrated that those who regularly walked around for 1 minute and 40 seconds had lower blood sugar and insulin levels than those who spent their day at their desk.52 Standing up every 10 minutes when sedentary is highly beneficial.
Grounding
“Earthing,” or grounding, is the act of making physical contact with electrons on the surface of the earth. Grounding has been found to stabilize many aspects of physiology and help regulate internal rhythms.53 One experiment found that earthing continually during both rest and physical activity over a 72-hour period decreased fasting glucose among patients with T2D.54
Personal Experiment
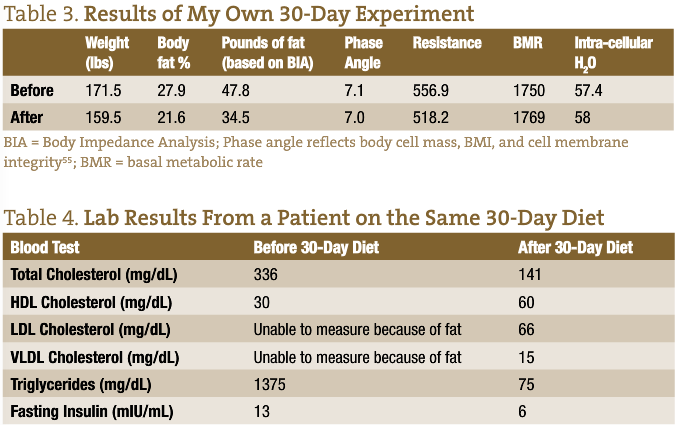
The author underwent his own version of a 30-day starch elimination diet (eliminating all concentrated forms of CHOs), and experienced remarkable results. Primary measuring tools were the Bio-Impedance Analysis (BIA) and a medical scale. (See Table 3 for results; Table 4 lists lipid results for a patient following the same diet)
Principles of the Diet
- The mostly anti-inflammatory, almost vegan, gluten-free, grain-free, 30-day diet consisted of: wild-caught salmon, berries, dark chocolate (85% cocoa), black and pinto beans, avocado, raw nuts and seeds, kale, garlic, eggs, occasional orange or apple, and herbs.
- The diet was high in fat (65-70%), which strongly delays hunger, prevents cravings, and hypoglycemia.
- Exact portion size for each food is determined after BIA determines the BMR. Calculate about 300 calories less than the BMR for daily caloric goal. I found that I never could eat my allotted portion because of the high proportion of fat.
Sleep
Growing evidence supports associations between chronic sleep loss, and the risk of obesity, insulin resistance, and T2D. Sleep loss of healthy young adults demonstrated marked alterations in glucose metabolism, including decreases in insulin sensitivity and glucose tolerance. Appetite regulation was also affected: leptin (which normally decreases appetite) was decreased, and ghrelin (which stimulates appetite) was increased. These changes resulted in increased hunger and appetite, which can lead to overeating and weight gain.56
 Dennis Godby, MA, ND has been interested in nutrition and running since he was a child. While studying exercise physiology and nutrition in college, he organized family “fun runs” in his college community to encourage exercise. He has made a solo run of 1420 miles over the Northern Cascades and Canadian Rockies. To raise media awareness about human rights in Central America, he ran from San Francisco to Washington, DC. He went on to found The Run: Moving Natural Medicine Forward, a 3000-mile transcontinental run to increase naturopathic medicine visibility (see www.TheRun.org). After graduating from NCNM at age 48, he founded the Diabetes Natural Path Center, a medical practice in Sacramento, CA, and has been practicing there since 2005. Witnessing his mother’s struggle with type 2 diabetes inspired Dr Godby to make a professional commitment to help fight the diabetes epidemic. Dr Godby wrote an e-book on diabetes in 2007: The Practical Guide to Overcoming Diabetes Naturally.
Dennis Godby, MA, ND has been interested in nutrition and running since he was a child. While studying exercise physiology and nutrition in college, he organized family “fun runs” in his college community to encourage exercise. He has made a solo run of 1420 miles over the Northern Cascades and Canadian Rockies. To raise media awareness about human rights in Central America, he ran from San Francisco to Washington, DC. He went on to found The Run: Moving Natural Medicine Forward, a 3000-mile transcontinental run to increase naturopathic medicine visibility (see www.TheRun.org). After graduating from NCNM at age 48, he founded the Diabetes Natural Path Center, a medical practice in Sacramento, CA, and has been practicing there since 2005. Witnessing his mother’s struggle with type 2 diabetes inspired Dr Godby to make a professional commitment to help fight the diabetes epidemic. Dr Godby wrote an e-book on diabetes in 2007: The Practical Guide to Overcoming Diabetes Naturally.
References
- Centers for Disease Control and Prevention. Power of Prevention. CDC Web site. http://www.cdc.gov/chronicdisease/resources/publications/index.htm. Accessed September 21, 2013.
- Ahima, RS, Lazar MA. Physiology. The health risk of obesity—better metrics imperative. Science. 2013;341(6148):856-858.
- Wei M, Gaskill SP, Haffner SM, Stern MP. Waist circumference as the best predictor of noninsulin dependent diabetes mellitus (NIDDM) compared to body mass index, waist/hip ratio and other anthropometric measurements in Mexican Americans–a 7-year prospective study. Obes Res. 1997;5(1):16-23.
- Gluck ME, Geliebter A, Lorence M. Cortisol stress response is positively correlated with central obesity in obese women with binge eating disorder (BED) before and after cognitive-behavioral treatment. Ann NY Acad Sci. 2004;1032:202-207.
- Dagogo-Jack S, Umamaheswaran I. Askari H. Leptin response to glucocorticoid occurs at physiological doses and is abolished by fasting. Obes Res. 2003;11(2):232-237.
- Otsuka R, Yatsuya H, Tamakoshi K, et al. Perceived psychological stress and serum leptin concentrations in Japanese men. Obesity (Silver Spring). 2006;14(10):1832-1838.
- Casanueva FF, Dieguez C. Neuroendocrine regulation and actions of leptin. Front Neuroendocrinol. 1999;20(4):317-363.
- Rouach V, Bloch M, Rosenberg N, et al. The acute ghrelin response to a psychological stress challenge does not predict the post-stress urge to eat. Psychoneuroendocrinology. 2007;32(6):693-702.
- Chaiopanont S. Hypoglycemic effect of sitting breathing meditation exercise on type 2 diabetes at Wat Khae Nok Primary Health Center in Nonthaburi province. J Med Assoc Thai. 2008;91(1):93-98.
- Paul-Labrador M, Polk D, Dwyer JH, et al. Effects of a randomized controlled trial of transcendental meditation on components of the metabolic syndrome in subjects with coronary heart disease. Arch Intern Med. 2006;166(11):1218-1224.
- Hayashi T, Murakami D. The effects of laughter on post-prandial glucose levels and gene expression in type 2 diabetic patients, Life Sci. 2009;85(5–6):185–187.
- Bernstein RK. Dr. Bernstein’s Diabetes Solution: A Complete Guide to Achieving Normal Blood Sugars. New York, NY: Little, Brown & Co; 1997:55.
- Murray M, Lyon M. How to Prevent and Treat Diabetes with Natural Medicine. New York, NY: Riverhead Books; 2003.
- Chandalia, M, Garg A, Lutjohann D, et al. Beneficial effects of high fiber dietary intake in patients with type 2 diabetes mellitus. N Engl J Med. 2000;342:1392-1398.
- Hagander B, Schersten B, Asp N, et al. Effect of dietary fibre on blood glucose, plasma immunoreactive insulin, C-peptide and GIP responses in non-insulin dependent (type 2) diabetics and controls. Acta Med Scand. 1984;21:205-213;
- Rendell M. Dietary treatment of diabetes mellitus. N Engl J Med. 2000;342(19):1440-1441.
- Liljeberg H, Björck I. Delayed gastric emptying rate may explain improved glycaemia in healthy subjects to a starchy meal with added vinegar. Eur J Clin Nutr. 1998;52(5):368-371.
- Jenkins DJ, Wolever TM, Taylor RH, et al. Slow release dietary carbohydrate improves second meal tolerance. Am J Clin Nutr. 1982;35(6):1339-1346.
- Gaby A. Diabetes mellitus. In: Nutritional Medicine. Concord, NH; 2011: 1083-1084.
- Zhang WQ, Wang HW, Zhang YM, Yang YX. [Effects of resistant starch on insulin resistance of type 2 diabetes mellitus patients]. Zhonghua Yu Fang Yi Xue Za Zhi. 2007;41(2):101–104.
- Johnston KL, Thomas EL, Bell JD, et al. Resistant starch improves insulin sensitivity in metabolic syndrome. Diabet Med. 2010;27(4):391–397.
- Vonk RJ, Hagedoorn RE, de Graaff R, et al. Digestion of so-called resistant starch sources in the human small intestine. Am J Clin Nutr. 2000;72(2):432–438.
- Robertson MD, Currie JM, Morgan LM, et al. Prior short-term consumption of resistant starch enhances postprandial insulin sensitivity in healthy subjects. Diabetologia. 2003;46(5):659–665.
- Robertson MD, Bickerton AS, Dennis AL, et al. Insulin-sensitizing effects of dietary resistant starch and effects on skeletal muscle and adipose tissue metabolism. Am J Clin Nutr. 2005;82(3):559–567.
- Robertson MD, Wright JW, Loizon E, et al. Insulin-sensitizing effects on muscle and adipose tissue after dietary fiber intake in men and women with metabolic syndrome. J Clin Endocrinol Metab. 2012;97(9):3326-3332.
- Maki KC, Pelkman CL, Finocchiaro ET, et al. Resistant starch from high-amylose maize increases insulin sensitivity in overweight and obese men. J Nutr. 2012;142(4):717–723.
- Penn-Marshall M, Holtzman GI, Barbeau WE. African Americans may have to consume more than 12 grams a day of resistant starch to lower their risk for type 2 diabetes. J Med Food. 2010;13(4):999–1004.
- Shen L, Keenan MJ, Raggio A, et al. Dietary-resistant starch improves maternal glycemic control in Goto-Kakizaki rat. Mol Nutr Food Res. 2011;55(10):1499-1508.
- Bodinham CL, Smith L, Wright J, et al. Dietary fibre improves first-phase insulin secretion in overweight individuals. PLOS One. 2012;7(7):e40834.
- Wiseman CE, Higgins JA, Denyer GS, Miller JC. Amylopectin starch induces nonreversible insulin resistance in rats. J Nutr. 1996;126(2):410–415.
- Byrnes SE, Miller JC, Denyer GS. Amylopectin starch promotes the development of insulin resistance in rats. J Nutr. 1995;125(6):1430–1437.
- Higgins JA, Brand Miller JC, Denyer GS. Development of insulin resistance in the rat is dependent on the rate of glucose absorption from the diet. J Nutr. 1996;126(3):596–602.
- Higgins JA, Higbee DR, Donahoo WT, et al. Resistant starch consumption promotes lipid oxidation. Nutr Metab (Lond). 2004;1(1):8.
- O’Dea K. Nestel PJ, Antonoff L. Physical factors influencing postprandial glucose and insulin responses to starch. Am J Clin Nutr. 1980;33(4):760-765.
- Najjar N, Adra N. Hwalla N. Glycemic and insulinemic responses to hot vs. cooled potato in males with varied insulin sensitivity. Nutr Res. 2004;24(12):993-1004.
- Goetz F, Bishop J, Halberg F, et al. Timing of single daily meal influences relations among human circadian rhythms in urinary cyclic AMP and hemic glucagon, insulin and iron. Experientia. 1976;32(8):1081-1084.
- Pan A, Sun Q, Manson JE, et al. Walnut consumption is associated with lower risk of type 2 diabetes in women. J Nutr. 2013;134(4):512-518.
- Tan SY, Mattes RD. Appetitive, dietary and health effects of almonds consumed with meals or as snacks: a randomized, controlled trial. Eur J Clin Nutr. 2013 Oct 2. doi: 10.1038/ejcn.2013.184. [Epub ahead of print]
- Guasch-Ferré M, Bulló M, Martínez-González MÁ, et al. Frequency of nut consumption and mortality risk in the PREDIMED nutrition intervention trial. BMC Med. 2013;11:164.
- Sargeant LA, Khaw KT, Bingham S, et al. Fruit and vegetable intake and population glycosylated hemoglobin levels: the EPIC-Norfolk Study. Eur J Clin Nutr. 2001;55:342-348.
- Karlsson FH, Tremaroli V, Nookaew I, et al. Gut metagenome in European women with normal, impaired and diabetic glucose control. Nature. 2013;498(7452):99-103.
- Swithers SE. Artificial sweeteners produce the counterintuitive effect of inducing metabolic derangement. Trends Endocrinol Metab. 2013;24(9):431-441.
- Bassett DR, Schneider PL, Huntington GE. Physical activity in an Old Order Amish community. Med Sci Sports Exerc. 2004;36(1):79-85.
- Food Research and Action Center. Overweight and Obesity in U.S. FRAC Web site. http://frac.org/initiatives/hunger-and-obesity/obesity-in-the-us/. Accessed September 23, 2013.
- Hood MS, Little JP, Tarnopolsky MA, et al. Low-volume interval training improves muscle oxidative capacity in sedentary adults. Med Sci Sports Exerc. 2011;43(10):1849–1856.
- Little JP, Gillen JB, Percival ME, et al. Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. J Appl Physiol (1985). 2011;111(6):1554-1560.
- Medical News Today. How to Get Fit With 3 Minutes of Exercise a Week: BBC Doc Tries “HIT.” MNT Web site. http://www.medicalnewstoday.com/articles/242498.php. Accessed September 21, 2013.
- Lira FS, Carnevali LC Jr, Zanchi NE, et al. Exercise intensity modulation of hepatic lipid metabolism. J Nutr Metab. 2012;2012:809576.
- Heydari M, Freund J, Boutcher SH. The effect of high-intensity intermittent exercise on body composition of overweight young males. J Obes. 2012;2012:480467.
- Grøntved A, Rimm EB, Willett WC, et al A prospective study of weight training and risk of type 2 diabetes mellitus in men. Arch Intern Med. 2012;172(17):1306-1312.
- Kiecolt-Glaser JK, Christian LM, Andridge R, et al. Adiponectin, leptin, and yoga practice. Physiol Behav. 2012;107(5):809–813.
- Dunstan DW, Kingwell BA, Larsen R, et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care. 2012;35(5):976-983.
- Chevalier G, Sinatra ST, Oschman JL, et al. Earthing: health implications of reconnecting the human body to the earth’s surface electrons. J Environ Public Health. 2012;2012:291541.
- Sokal K, Sokal P. Earthing the human body influences physiologic processes. J Altern Complement Med. 2011;17(4):301-308.
- Kumar S, Dutt A, Hemraj S, et al. Phase Angle Measurement in Healthy Human Subjects through Bio-Impedance Analysis. Iran J Basic Med Sci. 2012;15(6):1180-1184.
- Spiegel K, Knutson K, Leproult R, et al. Sleep loss: a novel risk factor for insulin resistance and Type 2 diabetes. J Appl Physiol (1985). 2005;99(5):2008-2019.

")















