
Tolle Causam
Eric Yarnell, ND, RH(AHG)
Inguinal herniation, a condition recognized in many ancient medical writings, occurs commonly in men, with a lifetime incidence of between 6% and 27%.1 Inguinal hernia repair is one of the top 3 most common surgical procedures in the developed world, although it is likely overused. Widespread hernia surgery commenced in 1865, once anesthesia and aseptic technique were commonplace.2
Inguinal hernias occur at a point of weakness in the anteroinferior abdomen known as the myopectineal orifice of Fruchaud. Direct, indirect, and femoral hernias all traverse this area, although they then take different pathways through the complex architecture of the abdominopelvic wall. Only femoral hernias, now known to be a subtype of inguinal hernia, occur more commonly in women than in men.
The age-old concern about distinguishing direct and indirect hernias by palpation in the office is essentially pointless and does not affect management decisions. Ultrasonography has poor sensitivity and specificity in assessing the presence and severity of inguinal hernias. When there is doubt, magnetic resonance imaging is the technique of choice.
Causes
The causes of inguinal herniation are not completely known. When occurring in infancy or childhood, a congenital defect of the abdominopelvic wall is usually suspected but is almost impossible to confirm. Some infants have a patent processus vaginalis.
Inguinal hernia is much more common in adults. Multiple factors have a role in causing inguinal hernia among them. Low-grade patent processus vaginalis and changes in aging connective tissue (possibly aggravated by smoking or chronic corticosteroid use) seem to be the main culprits.3 Though it has long been suggested obesity increases the risk of herniation due to increased intra-abdominal pressure, large modern trials4 suggest exactly the opposite.Microscopic assessment of tissue from patients who had inguinal hernias revealed decreased collagen density and a less ordered structure compared with patients who did not have hernias.5 Abnormal metalloproteinase activity is also associated with inguinal hernia formation, suggesting that the normal process of extracellular matrix remodeling is aberrant in patients with inguinal hernia.
The idea that acute intra-abdominal pressure predisposes to inguinal herniation is contradicted by many anatomical changes occurring during maneuvers that produce such pressures. Abdominopelvic wall strength is at its greatest during acute lifting and is weakest during relaxation. However, acute intra-abdominal pressures sufficient to overcome wall strength can contribute to herniation.
Various types of surgery and procedures affecting the region, including appendectomy, radical prostatectomy, and peritoneal dialysis, increase the risk of inguinal herniation. Connective tissue disorders such as polycystic kidney disease and Ehlers-Danlos syndrome are also known to do this.
A case-control study6 found that the lack of breastfeeding was a risk factor for severe inguinal hernia in Naples, Italy. The mechanism of this association is unknown.
Nonsurgical Treatment
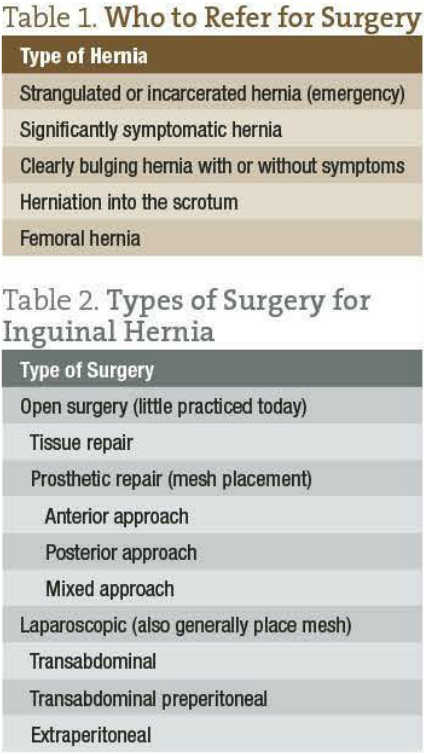 Many inguinal herniations are mild and do not require surgical intervention. The authors of a meta-analysis7 concluded that older men with asymptomatic or mildly symptomatic hernias do just as well with watchful waiting as with surgery. A survey8 of patients with incarcerated hernias in Cali, Columbia, led to the determination that the average 65-year-old man in that setting with an inguinal hernia has a 3.6% chance of its incarcerating by age 75 years. Research among somewhat younger men of predominantly white race/ethnicity supports this same contention.9 Taking some simple steps to help prevent worsening or acute strangulation of hernias in younger men may also reduce the risk of progression and the need for surgery, but research on this is sparse. These data must be balanced against the significantly higher incidence of mortality when hernias are treated emergently. Femoral hernias have a much higher risk of incarceration and should generally be treated surgically (Table 1 and Table 2).
Many inguinal herniations are mild and do not require surgical intervention. The authors of a meta-analysis7 concluded that older men with asymptomatic or mildly symptomatic hernias do just as well with watchful waiting as with surgery. A survey8 of patients with incarcerated hernias in Cali, Columbia, led to the determination that the average 65-year-old man in that setting with an inguinal hernia has a 3.6% chance of its incarcerating by age 75 years. Research among somewhat younger men of predominantly white race/ethnicity supports this same contention.9 Taking some simple steps to help prevent worsening or acute strangulation of hernias in younger men may also reduce the risk of progression and the need for surgery, but research on this is sparse. These data must be balanced against the significantly higher incidence of mortality when hernias are treated emergently. Femoral hernias have a much higher risk of incarceration and should generally be treated surgically (Table 1 and Table 2).
All men should be counseled in proper lifting technique, which includes exhaling during effort and thereby minimizing Valsalva maneuvers. If obese, they should be counseled to lose weight (or, more appropriately, to decrease adiposity). If smokers, they should be advised to stop.10
Improving connective tissue quality is a key goal in preventing and treating mild inguinal hernias. There is little (if any) research on the topic, but clinically this is likely why improvement in overall health through lifestyle changes is helpful. By eating more micronutrient-dense foods, improving the quality of ingested fats, and increasing exercise, patients build and maintain superior connective tissue over time.
Connective tissue tonics such as Equisetum arvense herb, Equisetum telmateia herb, and Centella asiatica whole plant may further improve the quality of impaired abdominopelvic wall matrix and prevent degradation. These herbs may also help with healing if surgical repair becomes necessary.
Redox-modulating herbs are generally considered more cardiovascular tonics but may be useful by improving the quality of the matrix material in blood vessels of the heart. These include Vaccinium myrtillus fruit, Aesculus hippocastanum seed, Collinsonia canadensis whole plant, and Crataegus species leaf, fruit, and flower. However, these agents act slowly and are unlikely to work without improvement in lifestyle factors.
Direct mechanical reduction of mild to moderate inguinal herniations is possible. Only light pressure should be used and over a large area, not a small point. This approach will not likely permanently reduce the lesion. The use of a truss is another option. This device is strapped around the waist and groin to put pressure against the affected area, preventing herniation. However, these tend to be uncomfortable and unappealing and are no longer widely used because of patient rejection of the treatment. For some patients without such inhibitions, this could be an effective option. It is also a traditional yoga practice to have a patient stand on his head.
 Eric Yarnell, ND, RH is a graduate of Bastyr University. He completed a two-year residency with Silena Heron, ND, and served as chair of botanical medicine at SCNM. He is past senior editor of the Journal of Naturopathic Medicine. Dr. Yarnell is a founding member and current president of the Botanical Medicine Academy and author of numerous textbooks and articles, including Naturopathic Urology and Men’s Health, Naturopathic Gastroenterology and Clinical Botanical Medicine. His area of clinical focus is urology and men’s health. He is assistant professor in botanical medicine at Bastyr University. Contact: 3670 Stone Way N, Seattle WA 98103; 425-602-3289; www.dryarnell.com.
Eric Yarnell, ND, RH is a graduate of Bastyr University. He completed a two-year residency with Silena Heron, ND, and served as chair of botanical medicine at SCNM. He is past senior editor of the Journal of Naturopathic Medicine. Dr. Yarnell is a founding member and current president of the Botanical Medicine Academy and author of numerous textbooks and articles, including Naturopathic Urology and Men’s Health, Naturopathic Gastroenterology and Clinical Botanical Medicine. His area of clinical focus is urology and men’s health. He is assistant professor in botanical medicine at Bastyr University. Contact: 3670 Stone Way N, Seattle WA 98103; 425-602-3289; www.dryarnell.com.
References
Primatesta P, Goldacre MJ. Inguinal hernia repair: incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol. 1996;25(4):835-9.
Anonymous. Inguinal hernia in the 21st century: an evidence-based review. Curr Probl Surg. 2008;45:261-312.
van Veen RN, van Wessem KJ, Halm JA, Simons MP, Plaisier PW, Jeekel J, Lange JF. Patent processus vaginalis in the adult as a risk factor for the occurrence of indirect inguinal hernia. Surg Endosc. 2007;21:202–205.
Rosemar A, Angerås U, Rosengren A. Body mass index and groin hernia: a 34-year follow-up study in Swedish men. Ann Surg. 2008;247(6):1064-8.
Klinge U, Binnebosel M, Mertens PR. Are collagens the culprits in the development of incisional and inguinal hernia disease? Hernia. 2006;10(6):472-477.
Pisacane A, de Luca U, Vaccaro F, et al. Breast-feeding and inguinal hernia. J Pediatr. 1995;127:109-111.
INCA Trialists Collaboration. Operation compared with watchful waiting in elderly male inguinal hernia patients: a review and data analysis. J Am Coll Surg. 2011;212(2):251-259.e1-4.
Neutra R, Velez A, Ferrada R, Galan R. Risk of incarceration of inguinal hernia in Cali, Colombia. J Chronic Dis. 1981;34:561-564.
Fitzgibbons RJ Jr, Giobbie-Hurder A, Gibbs JO, et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. JAMA. 2006;295(3):285-292.
Cannon DJ, Read RC. Metastatic emphysema: a mechanism for acquiring inguinal herniation. Ann Surg. 1981;194(3):270-278.

")


















