
Tolle Causam
Iva Lloyd, BScH, RPE, ND
Consciousness plays a tremendous role in both objective and subjective health status, but the understanding of how it is formed continues to be an area of great debate and mystery. New advances in physics are shedding some light on this evasive aspect of man. Science is starting to understand the neuroplastic mechanisms of the brain and its ability to form objective reality and streams of consciousness. The other area of research that is receiving a great degree of attention is the role of the senses and other filtering systems of the body and how this bidirectional interplay between a person’s environment and his or her subjective awareness provides a framework for the formation of consciousness.1
This paper will examine how consciousness is impacted by a number of filters and protective barriers. This protection is afforded by the physical and non-physical senses and the mucous and epithelial membranes, which collectively act as the filtering systems of the body. They are protective barriers to both subjective and objective health and, to a large degree, determine a person’s state of consciousness. A growing concern is that the filtering systems become overwhelmed due to lifestyle factors, environmental toxins, and the intensity and frequency of stimuli with which they have to deal. I contend that the filtering systems of the body represent the rate-limiting step between health and disease, both objectively and subjectively (Figure 1).
Figure 1: The Role of Filters in Health and Disease
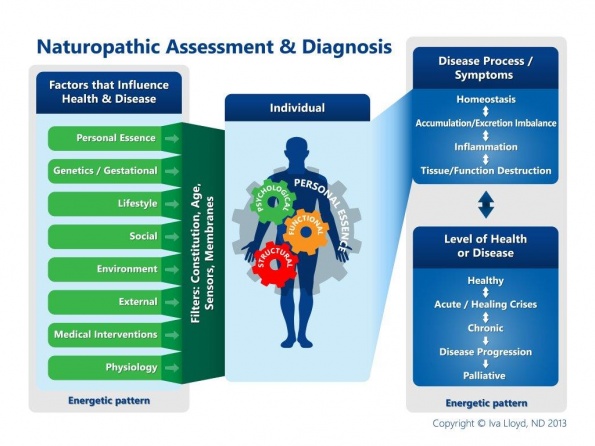
Sensors and filters determine what gets in and what gets out. When strong, they restrict the entry of toxins and foreign substances and they protect the body from being overwhelmed by excess information and external stimuli. They influence biochemical processes and influence the rate and state of aging. They determine the degree of “protection” and “communication” an individual has with their external world. In short, they determine a person’s perception of their environment, their resiliency and their state of health.
<!––nextpage––>
The Senses
Consciousness refers to one’s subjective awareness of their surrounding world, of the self, and of one’s thoughts and feeling, the subjective qualities of phenomenal experience, as well as sensations, feelings, perceptions, volitions, desires, and mental images.2,3 It is affected by the physical and non-physical senses (Figure 2).
Figure 2. Information exchange between consciousness and its source
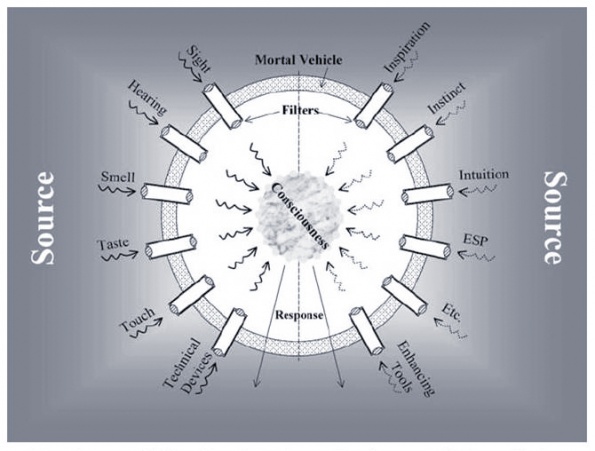
- Physical senses are the initial sensors or filters of the body. They include the eyes, ears, nose, mouth, and skin, and hence relate to vision, hearing, smell, taste and touch, respectively. The physiological structures of the senses are some of the most complex structures in the body.
- The non-physical senses include inspiration, instinct, intuition, ESP, etc. The biophysical architectures and the neurological and biochemical processes by which the sensors execute their functions have been broadly and deeply studied, yet considerably less insight has been achieved regarding their roles in establishing the subjective qualities of life.1
Physical sensors are constantly acquiring information about their environment. The intricate design of the brain is then able to interpret and respond to this input in a specific manner. The sensors are designed, if functioning optimally, to “sense” or “read” all input that they encounter. Even the shape of the senses have a specific purpose. For example, the eyes are positioned to take in what is going on in front of a person, with the emphasis on peripheral and forward visual input; the ears are best at picking up lateral sounds, the nose is best at picking up smells that are right under the nose, etc. Every sense is then designed to filter out irrelevant information through multiple steps and physiological features. Much of the filtering is based on awareness, expectations and past experiences. Input from the senses is converted to specific wave patterns or resonance patterns which are then interpreted by the brain. A person’s perception depends on the simultaneous, cooperative activity of millions of neurons spread throughout the cortex and on a person’s current state of consciousness. Based on that interpretation, the mind/body activates a response or reaction. The intuitive and analytical awareness of this composite creates a subjective awareness or consciousness (terms which will be used interchangeably throughout this document), which then influences how one interacts with their environment.
All senses have physical restrictions that determine the range and frequency of stimuli that they can sense. They all have a specific bandwidth or specific capacity of interpretation. For example, the eyes only objectively perceive the narrow band of electromagnetic radiation, from 400 to 700 nanometers in wavelength, and are oblivious to the much more extensive infrared and ultraviolet domains. Ears respond to a narrow range of acoustic frequencies without the objective awareness of infrasonic and ultrasonic sounds. Taste, smell and the sense of touch are sensitive only to tiny portions of the chemical range that is available. With mindfulness and expectations, one can increase their awareness of environmental stimuli. For example, an artist has increased perception of color and depth, a musician is able to distinguish the subtleties in music, and a surgeon or body worker is generally extra sensitive to changes in the tone and texture of bodily tissues. Development of the psychical modalities, such as intuition, instinct and inspiration, has also been proven to increase a person’s awareness and breadth of input.1
Consciousness is based on both the physiological processing of the brain and on a person’s level or state of consciousness at the time of exposure. From an objective perspective, physical senses are affected by the intensity of the stimuli, the frequency of stimuli, and the range of stimuli. Subjectively, they are affected by cognitive bias, cultural bias, and intention. Processing sensory information is based on past experiences, current state of awareness, expectations, and present state. Senses involve two-way communication, which is constantly enhanced, changed, and influenced by experiences and by training. Their resiliency is a reflection of both objective and subjective exposure.
Input from the senses, at any point-in-time, is reflected in a person’s self-awareness of both themselves and their current environment. This awareness changes constantly and is influenced by both factors within our awareness and outside of our awareness. Two of the most studied senses, with respect to consciousness or subjective awareness, include vision and hearing.
Vision
The concept of visual consciousness cannot be explained by the current neurophysiological, psychophysical, and psychological approaches to vision. New research proposes that seeing occurs when a person exploring the environment has mastered the governing laws of “sensorimotor contingency,” which provides a principled means of accounting for visual consciousness.4 It also provides support for the concepts of sensorimotor adaptation, visual stability despite eye movements, visual “filling in,” (eg, compensation for ‘blind spots’), change blindness, sensory substitution, and the perception of color. Brain processes participate in seeing, but do not deserve to be thought of as “the locus of seeing in the brain.” Seeing is something we do, not something that happens in our brains.4
Subjective vision is strongly correlated with quality of life, especially in the older individuals. The value older individuals attach to their lives is significantly influenced by their visual capacity.5 Roughly 20% of individuals over 65 years of age have trouble with their vision, even with corrective glasses and lenses. Poor subjective vision contributes to depressive symptoms and lower mental health directly and indirectly by restricting an individual’s ability to carry out routine day-to-day physical activities and increasing their feelings of social isolation. Objective vision contributes significantly to physical and driving limitations but is generally unrelated to feelings of social isolation or depressive symptomatology.5
Hearing
Selective hearing is one of the most commonly accepted aspects of the senses that relates to how a person’s expectations and current state of awareness affects what they hear. Selective hearing is about focusing attention on a source of interest, analyzing the acoustic scene, and forming a perceptual auditory awareness. Much of how people interact in a social setting is based on selective hearing. Fine-tuning hearing skills, such as music training, can enhance cognitive and language-related skills, such as deciphering speech in background noise, which are critical to the success of a person, academically, emotionally, and vocationally.6
Changes in hearing ability, or peripheral degradations in sound recognition, impact a person’s ability to pick up or recognize auditory cues such as location, pitch and timbre of the auditory input. Degraded peripheral processing increases the time required to form auditory awareness, to focus selective attention, and to switch attention from one auditory sound to another (a skill that is used, for example, when trying to participate in a lively conversation). Hearing deficits interfere with strategies that normal-hearing listeners employ in complex acoustic settings, including the use of memory to fill in bits of a conversation that are missed.
Overall hearing deficits, like vision, are associated with decreased quality of life, especially in older adults. Approximately one-third of adults 61 to 70 years of age, and more than 80% of those older than 85 years of age, experience hearing loss. Men generally experience greater hearing loss and have an earlier onset compared with women.7 Hearing loss associated with aging, referred to as presbycusis, is the most common sensory deficit in the elderly and is becoming a serious social and health problem. Hearing loss impairs the exchange of information, which adversely impacts everyday life by inducing loneliness, isolation, frustration, dependence, and communication disorders.8
Decreased sensory ability is not only a consideration for the elderly. What people listen to and see affects their reality, their development, and how they interact with their environment at all ages. For example, research with younger children and teenagers shows that exposure to social media affects a person’s well-being and development and that it can contribute to fears and anxieties in children, depending on the content. Both fictional and news programming can cause persistent emotional upset, thereby affecting a child’s social development. Violent television shows and video games are associated with desensitization to violence and in an increase in aggressive behaviour, whereas educational programs can increase a child’s cooperation, altruism, and tolerance for others.9,10
Breakdown of the Filters
When the senses are resilient, they are protective and are supportive of health. A weakening in this resiliency results in shifts in consciousness, as well as decreases in the subjective awareness of a person’s environment and their quality of health. The following illustrates the broad range of factors that affect the integrity and resiliency of the filtering systems of the body.
- Nutritional imbalances and deficiencies weaken the senses. A deficiency of zinc, for example, is associated with abnormalities in taste and smell, changes in cognition, and cerebellar dysfunction.11
- Recognition of a gut-brain barrier link is becoming more widely accepted as research illustrates, for example, that mental disorders such as depression can be linked to intestinal mucosal dysfunction.12 Other research indicates an increased IgA and IgM response against intestinal commensals in chronic depression.13
- The intestinal epithelial membrane regulates nutrients absorption, water and ion fluxes, and represents the first defensive barrier against toxins and enteric pathogens. Tight junctions between the epithelial cells reduce the paracellular space and the passage of charge entities, while forming a physical barrier to lipophilic molecules. Exposure to mild irritants, proinflammatory cytokines, toxins and pathogens, and adverse environmental conditions can open these tight junctions, increasing paracellular permeability. Intestinal barrier dysfunction is associated with various intestinal and non-intestinal disorders, including diarrheal infection, inflammatory bowel disease, and celiac disease.14
- There is some thought, largely based on animal studies, that genetically modified foods can contribute to intestinal dysfunction and may even penetrate the blood-brain barrier.15 Exposure to electromagnetic fields is also known to disrupt the blood-brain barrier.16,17
- Although exposure to mold has been associated with depression, a person’s perception of control over their environment has been shown to significantly moderate this association, independent of the actual health-risk that exists.18
- The eyes are designed to protect the body, yet they are at risk of injury by direct exposure to airborne pollutants, to splash injury from chemicals, and to exposure to blood-borne toxins. Drugs and environmental toxins can also compromise vision by damaging the visual nervous system.19
- A reduced sense of smell can significantly impair one’s quality of life by altering hygiene, disrupting appetite and taste, inducing changes in weight due to reduced pleasure in eating, or making it more difficult to avoid health risks associated with spoiled food or leaking natural gas. It can also result in changes in emotional and sexual behavior. Loss of smell is greatest in the elderly. Possible causes include head trauma, oxidative stress, changes in the saliva or fluids bathing the olfactory mucosa, autoimmunity, pharmaceutical drugs, recreational drugs, surgeries and radiation, viral infections, poor dietary habits and toxic exposure to chemicals and odors. Prescription medications are a common cause of taste impairment.20,21,22
- Excessive exposure to very noisy environments can cause noise-induced hearing loss (NIHL). Cigarette smoking can also adversely affect hearing and can worsen NIHL in those exposed to high noise levels for longer than 10 years. The effects of smoking and high noise level exposure appear to be additive.23 Other factors that are commonly associated with hearing loss include obstruction (including cerumen) and use of ototoxic medications.
- Urinary concentrations of cadmium, molybdenum, and tungsten, which are commonly linked with heart disease, have also been associated with vision disorders. Urinary 2,4,5-trichlorophenol and arsenic acid concentrations and circulating mono-n-butyl phthalate, mono-benzyl phthalate, and mono-(3-carboxypropyl) phthalate metabolites have also been linked with hearing disorders. Urinary barium and 4-tert-octyl-phenol concentrations have been associated with balance disorders. Higher urinary concentrations of barium, 2,4-dichlorophenol, and mono-benzyl phthalate have been noted in individuals who had experienced ringing, roaring, or buzzing in their ears during the previous year.24
Conclusion
The integrity of the senses is critical to optimal health. The breakdown of the physical senses may actually be the rate-limiting step between health and disease. Minimizing the bombardment of the senses by constant noise, light and smells is a start. Decreasing the exposure to EMF radiation, genetically modified foods, environmental toxins and chemicals is also necessary. Focusing on the healing of epithelial and mucous membranes should be an integral part of every treatment plan. Most importantly, it is about looking at health and consciousness from the perspective of the body’s ability to filter and protect itself as it is in constant interplay with its external environment.
 Iva Lloyd, BScH, RPE, ND founded Naturopathic Foundations Health Clinic in 2002 after graduating from the Canadian College of Naturopathic Medicine (CCNM). Her focus is on identifying the factors contributing to disease and understanding their physiological and energetic patterns. She is known for her patience, knowledge and ability to guide patients through a life transformation.
Iva Lloyd, BScH, RPE, ND founded Naturopathic Foundations Health Clinic in 2002 after graduating from the Canadian College of Naturopathic Medicine (CCNM). Her focus is on identifying the factors contributing to disease and understanding their physiological and energetic patterns. She is known for her patience, knowledge and ability to guide patients through a life transformation.
She has studied many different healing systems. Dr. Lloyd is a registered polarity therapist and educator and a Reiki master.
She is editor of the professional journal of the CAND, and she is on the editorial board of other professional journals. She teaches part-time at the CCNM and she presents internationally on naturopathic assessments, the energetics of health, and the role of the mind in healing.
References
1. Jahn RG, Dunne BJ. Sensors, Filters and the Source of Reality. J of Sci Explor. 2004;18(4):547-570.
2. Sommerhoff G, MacDorman K. An account of consciousness in physical and functional terms: a target for research in the neurosciences. Integr Physiol Behav Sci. 1994;29(2):151-181.
3. Hameroff S. Consciousness, the brain, and spacetime geometry. Ann NY Acad Sci. 2001;929:74-104.
4. O’Regan JK, Noë A. A sensorimotor account of vision and visual consciousness. Behav Brain Sci. 2001;24(5):939-973.
5. Bookwala J, Lawson B. Poor vision, functioning, and depressive symptoms: A test of the Activity Restriction Model. Gerontologist. 2011;51(6):798-808.
6. Strait D, Kraus N. Playing Music for a Smarter Ear: Cognitive, Perceptual and Neurobiological Evidence. Music Percept. 2011;29(2):133-146.
7. Walling AD, Dickson GM. Hearing loss in older adults. Am Fam Physician. 2012;85(12):1150-1156.
8. Ciorba A, Bianchini C, Pelucchi S, Pastore A. The Impact of hearing loss on the quality of life of elderly adults. Clin Interv Aging. 2012;7:159-163.
9. Funk JB. Children’s exposure to violent video games and desensitization to violence. Child Adolesc Psychiatr Clin N Am. 2005;14(3):387-404, vii-viii.
10. Wilson BJ. Media and children’s aggression, fear and altruism. Future Child. 2008;18(1):87-118.
11. Henkin RI, Patten BM, Re PK, Bronzert DA. A syndrome of acute zinc loss. Cerebellar dysfunction, mental changes, anorexia, and taste and smell dysfunction. Arch Neurol. 1975;32(11):745-751.
12. Maes M, Kubera M, Leunis JC. The gut-brain barrier in major depression: intestinal mucosal dysfunction with an increased translocation of LPS from gram negative enterobacteria (leaky gut) plays a role in the inflammatory pathophysiology of depression. Neuro Endocrinol Lett. 2008;29(1):117-124.
13. Maes M, Kubera M, Leunis JC, Berk M. Increased IgA and IgM responses against gut commensals in chronic depression: further evidence for increased bacterial translocation or leaky gut. J Affect Disord. 2012;141(1):55-62.
14. Catalioto RM, Maggi CA, Giuliani S. Intestinal epithelial barrier dysfunction in disease and possible therapeutical interventions. Curr Med Chem. 2011;18(3):398-426.
15. Institute for Responsible Technology. 65 Health risks of GM Foods. http://www.responsibletechnology.org/gmo-dangers/65-health-risks/5notes. Accessed April 15, 2013.
16. Nittby H, Grafström G, Eberhardt JL, et al. Radiofrequency and extremely low-frequency electromagnet field effects on the blood-brain barrier. Electromagn Biol Med. 2008;27(2):103-126.
17. Ding GR, Qiu LB, Wang XW, et al. EMP-induced alterations of tight junction protein expression and disruption of the blood-brain barrier. Toxicol Lett. 2010;196(3):154-160.
18. Shenassa Ed, Daskalakis C, Liebhaber A, et al. Dampness and mold in the home and depression: an examination of mold-related illness and perceived control of one’s home as possible depression pathways. Am J Public Health. 2007;97(10):1893-1899.
19. McCaa CS. The eye and visual nervous system: anatomy, physiology and toxicology. Environ Health Perspect. 1982;44:1-8.
20. Gaines AD. Anosmia and hyposmia. Allergy Asthma Proc. 2010;31(3):185-9.
21. Schiffmann SS. Taste and smell in disease (second of two parts). N Engl J Med. 1983;308(22):1337-1343.
22. Raviv JR, Kern RC. Chronic sinusitis and olfactory dysfunction. Otolaryngol Clin North Am. 2004;37(6):1143-1157, v-vi.
23. Tao L, Davis R, Heyer N, et al. Effects of cigarette smoking on noise-induced hearing loss if workers exposed to occupational noise in China. Noise Health. 2013;15(62):62-72.
24. Shiue I. Urinary environmental chemical concentrations and Vitamin D are associated with vision, hearing, and balance disorders in the elderly. Environ Int. 2013;53:41-6.
















