")
Dr. Carolyn Mukai, ND, Dr. Lynn Klassen, ND, Dr. Ece Toprak, ND
Expanding recognition of infection-triggered neuroinflammation in children, adolescents, and adults—and the evolving role of integrative immune regulation.
Abstract:
This clinical commentary examines the expanding understanding of Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS) and PANDAS as part of a broader spectrum of post-infectious neuroimmune syndromes. It reviews infectious triggers, immune mechanisms, autonomic and systemic features, and integrative management strategies while emphasizing the need to recognize these patterns beyond childhood.
Introduction: When Infection and Psychiatry Intersect
Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS) and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections (PANDAS) sit at a crossroads familiar to naturopathic clinicians: infection, immune dysregulation, neuroinflammation, and mental health. These conditions challenge the traditional separation between psychiatric and medical illness and highlight how immune activation following infection can abruptly reshape cognition, behavior, and emotional regulation.1-5
There is a growing body of clinical evidence that emphasizes the need for an integrative approach to these conditions. PANS and PANDAS offer a clear example of post-infectious syndromes, paralleling emerging models seen in long COVID and autoimmune neurologic disease.4, 5 Although classically described in pediatric populations, increasing evidence suggests that similar post-infectious neuropsychiatric presentations can occur in adolescents and adults, underscoring the importance of recognizing this pattern across the lifespan.6-8
A Child Who Changes Overnight
An eight-year-old child presents with sudden onset of tics, compulsive handwashing, separation anxiety, nightly rage episodes, and refusal to eat perceived unsafe foods. Within days, new bedwetting and profound insomnia appear. Four weeks earlier, the child had a febrile sore throat treated at home.
Subsequent evaluation reveals recent streptococcal exposure. Over the following months, symptoms flared with viral illnesses and sinus infections.
Infections as Triggers
The vignette above describes the classic clinical history and neuroimmune symptoms seen in PANDAS. Group A Streptococcus remains the best-studied trigger for PANDAS specifically, with symptom flares often following pharyngitis and partial response to antibiotics.2,4 However, this narrow definition has had to shift significantly since its inception due to increasing cases of similar, abrupt-onset neuropsychiatric syndromes without clear associations with streptococcal infections and onset extending into adolescence and adulthood. 1, 4-6
PANS is now the larger umbrella diagnosis that envelops PANDAS while broadening the landscape to include other possible inciting infections like Mycoplasma pneumoniae, Epstein-Barr virus, other viral/bacterial upper respiratory infections, Borrelia burgdorferi, and more recently COVID-19.4, 5
Research is still developing in this area, and it is likely that there are many other infectious triggers – especially infections that tend to go undiagnosed like Bartonella species infection and other vector borne illnesses. Bartonella species, as well as Borrelia species, are particularly indicated in infection-immune mediated neuropsychiatric symptoms throughout the lifespan that can overlap significantly with PANS.6-12
PANS diagnostic frameworks have also evolved to consider non-infectious triggers that may synergize with infections, including pre-existing immune disorders (autoimmunity, allergic/atopic disease), environmental exposures (for example, mold/mycotoxins in clinical practice) and psychosocial or physiologic trauma.1,4,5
Rather than a single‑pathogen syndrome confined to pre‑pubescent children, PANS is better conceptualized as a multi‑trigger immune vulnerability framework without strict age limits for diagnosis.1,4,5 The removal of the age restriction in characterizing these conditions is critical – as there are currently no well‑established, analogous models for infection mediated neuropsychiatric presentations in adolescents and adults, which are therefore at higher risk of misdiagnosis as primary psychiatric disorders.5-8
Emerging data suggests that similar post‑infectious neuroimmune phenomena may extend into adolescence and adulthood. Case reports and cohort studies now link vector‑borne infections such as Bartonella species and Lyme‑associated pathogens with persistent neuropsychiatric symptoms, including psychosis, mood changes, cognitive decline, and PANS‑like presentations in older patients.6-12 These findings, while preliminary, support viewing PANS and related post‑infectious neuroimmune syndromes along a lifespan continuum rather than as strictly pediatric conditions.5-8, 12
From Infection to Neuroinflammation
Proposed mechanisms in PANS include immune cross-reactivity between infectious and neuronal antigens (molecular mimicry) and the development of neuronal autoantibodies.3-5 Other described mechanisms include Th17 driven pro-inflammatory cytokine elevation, blood brain barrier disruption, microglial activation, and a shift towards pro-inflammatory innate immune responses.3-5 These immune processes are thought to affect dopaminergic signaling and basal ganglia circuits involved in behavior and emotion regulation.3-5 This model helps explain the wide spectrum of symptoms seen in PANS, including more overt neurologic changes like abnormal movement patterns (for example Sydenham chorea, also associated with streptococcal infection) and developmental regression in speech and handwriting.3-5 Neurodivergent traits are also common in this patient subset and may wax and wane with other neuroinflammatory symptoms.5
Other prominent symptoms may include abrupt eating restriction, sensory hypersensitivity, headaches, pain, insomnia, fatigue, cognitive dysfunction, and urinary disturbances. These systemic features distinguish PANS from primary psychiatric disorders and reflect widespread inflammation and autonomic dysfunction.1,4,5
Clinical Management Considerations
Expert consensus supports targeted antimicrobial therapy when infection is clearly identified in PANDAS presentations. For PANS, guidelines recommend a thorough infection exposure and family medical history with additional testing and treatment for well-characterized infectious and immune contributors.1-3
At the same time, expert opinions diverge on empiric antimicrobial therapy and on how broadly to screen for infections beyond standard diagnostic work‑ups for known triggers.
In our clinical experience, and based on emerging evidence, a detailed exposure and infection history is essential, and routine consideration of vector‑borne and associated infections (for example, Lyme disease and co‑infections) is warranted in appropriate epidemiologic contexts, particularly given the increasing prevalence of ticks and other vectors.6-8, 12,13
Immunotherapy is the common denominator in an integrative treatment approach as infections and other immune insults (for example, allergic phenomena, mast cell activation syndrome, environmental exposures) are addressed. 1-3, 5 Short courses of NSAIDs may reduce symptom burden without the degree of immune suppression associated with corticosteroids – an appealing option when chronic or persisting infection is suspected, though this remains controversial.3,13 Low dose naltrexone is another potential tool with theoretical data to support its neurologic immunomodulatory activity and with a favorable safety profile in children and adults despite lacking specific data in PANS or PANDAS. 13-15 Other immunomodulatory therapies such as corticosteroids and IVIG are also used in select cases and may be especially considered after treating identifiable infections and exposures.1-3
Additional integrative strategies focus on supporting immune regulation, blood brain barrier integrity, microbiome health, nutritional optimization, sleep restoration, and nervous system stabilization.1,4,5
Case Example – Tying It All Together
An 8‑year‑old female presented with a two‑year history of abrupt, multi‑system symptoms: chronic pain, dysarthria, anxiety/panic, developmental regression (speech, handwriting, oppositional behavior), sensory hypersensitivity, self‑stimulatory behaviors, tremor, abnormal gait, sleep disturbance, palpitations, and lymphadenopathy. Symptoms consistently improved with ibuprofen. She had a prior tick bite (treated briefly, standard Lyme serology negative) and recurrent respiratory/ENT symptoms.
Hospital neurology and rheumatology workup was largely unrevealing aside from low neutrophils, low C3, elevated TSH with normal T4, CMV IgG positivity, and sinus bradycardia. She was diagnosed with functional neurologic disorder/psychosomatic symptoms after major structural pathology was excluded via conventional lab testing (despite abnormalities). Private testing later showed weak T‑cell responses to Borrelia burgdorferi and Mycoplasma pneumoniae.
In our clinic, expanded infectious and metabolic testing revealed positive Borrelia IgG, indeterminate Bartonella serology, strong T‑cell response to latent CMV, and organic acid patterns suggesting yeast overgrowth, mitochondrial dysfunction, and altered neurotransmitter metabolism via private labs. Without clear OCD or food restrictions, technically this patient did not meet the criteria for PANS diagnosis, broadening the differential diagnosis.
We adopted a working diagnosis of PANS/autoimmune encephalitis with basal ganglia involvement in the context of suspected chronic/past tick‑borne infection, latent viral immune activation, and possible yeast/fungal dysbiosis. Treatment included staged neuro‑anti‑inflammatory and foundational support (omega‑3s, quercetin/vitamin C, mitochondrial and mineral support, cautious drainage/binders) followed by azithromycin plus cefuroxime and nystatin. This produced partial but meaningful improvement in pain and neurologic symptoms, with near‑resolution after additional traditional plant‑medicine care via external practitioner. Two years later, following a viral illness, she relapsed with migrating joint pain and sleep disturbance/fatigue; restarting mitochondrial and herbal neuro‑anti‑inflammatory support plus an initial trial with low‑dose naltrexone led to improved pain, sleep, and mood.
The Naturopathic Role
Although mechanistic understanding of PANS has progressed, there are still no well-validated laboratory markers to confirm the diagnosis. Clinicians must rely heavily on history and clinical presentation, and because psychiatric symptoms often dominate, many children and adolescents are given primary psychiatric or behavioral diagnoses. 1,4-6
This is despite concurrent, and very tangible, neurologic and systemic findings. These symptoms may then be considered psychosomatic symptoms or more broadly diagnosed as a functional neurologic disorder.
Patients and their families often seek second opinions at this stage – which is when you are most likely to encounter them in naturopathic practice. These alternative labels typically do not reflect the abrupt onset, multi‑system involvement, or the lived experience of patients and caregivers grappling with neuroimmune disease.
Naturopathic clinicians are uniquely positioned to recognize these patients early by using a whole‑person, pattern‑based approach rather than siloed organ systems and without age bias from diagnostic algorithms. Once you have seen this pattern, it becomes difficult to overlook in future cases. We are also well placed to think beyond conventionally recognized triggers, including considering additional infectious drivers (especially tick‑ and vector‑borne infections with more sensitive testing) that may contribute to persistent neuroimmune activation.
Clinical Pearls
- Sudden-onset neuropsychiatric symptoms – especially obsession-compulsion, severe food restriction, behavioral changes, or tics accompanied by systemic symptoms – should prompt a thorough immune and infection history.
- Systemic features may include abnormal movements, developmental regression in speech or writing, pain, fatigue, urinary frequency/incontinence, insomnia, and neurodivergent traits
- Infectious and non-infectious factors (autoimmunity, atopy, environmental exposures, psychosocial stress) can act in combination to drive neuroimmune dysfunction underlying PANS/PANDAS
- Early recognition can improve outcomes – especially in cases with clear temporal associations with infection or exposures
- Core management is twofold: identifying + treating contributing triggers while implementing immune-modulating and anti-inflammatory strategies.• While classically described in pediatrics, PANS diagnostic criteria do not include strict age cut-offs and similar post‑infectious neuroimmune presentations can emerge in adolescents and adults.
- Consider that additional infectious triggers and persistent infections may present as PANS – or as broader post‑infectious, immune‑mediated neuropsychiatric syndromes – that likely remain underrecognized from adolescence into adulthood
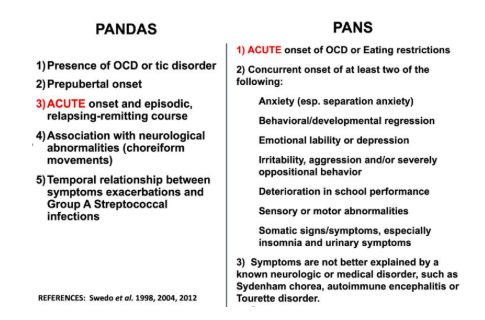
Diagnostic Criteria – PANS vs. PANDAS:
Swedo S, Menendez CM, Cunningham MW. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) 2024 Jul 7 [Updated 2024 Sep 13]. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]. 2nd edition. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2022 Oct 8. Chapter 26. Available from: https://www.ncbi.nlm.nih.gov/books/NBK607260/”
 Dr. Carolyn Mukai, ND is a licensed naturopathic physician with specialized training in vector-borne illness, chronic complex disease, and multidisciplinary care for Lyme disease and associated infections. She completed Canada’s first CNME-accredited residency program focused on vector-borne illness and chronic complex disease at Tandem Clinic, where she now treats patients using individualized assessment and integrative therapeutics. Dr. Mukai combines advanced lab evaluation, botanical and nutrient therapy, lifestyle medicine, and collaborative care to investigate underlying contributors to chronic conditions and support patient-centered, root-cause healing. She is also a speaker and educator on chronic infection strategies and practitioner education.
Dr. Carolyn Mukai, ND is a licensed naturopathic physician with specialized training in vector-borne illness, chronic complex disease, and multidisciplinary care for Lyme disease and associated infections. She completed Canada’s first CNME-accredited residency program focused on vector-borne illness and chronic complex disease at Tandem Clinic, where she now treats patients using individualized assessment and integrative therapeutics. Dr. Mukai combines advanced lab evaluation, botanical and nutrient therapy, lifestyle medicine, and collaborative care to investigate underlying contributors to chronic conditions and support patient-centered, root-cause healing. She is also a speaker and educator on chronic infection strategies and practitioner education.
 Dr. Lynn Klassen, ND is a licensed naturopathic physician and founder of Tandem Clinic, where she focuses on Lyme disease, chronic infection, and complex chronic illness using an integrative and systems-based clinical framework. As a Lyme Literate ND (LLND), she is trained in contemporary diagnostics and treatment strategies for challenging infectious and autoimmune presentations and has developed Canada’s first CNME-accredited naturopathic residency in vector-borne illness and chronic complex disease. Dr. Klassen is passionate about improving recognition and care for patients often overlooked by conventional systems and contributes to clinician education and training in chronic infection management.
Dr. Lynn Klassen, ND is a licensed naturopathic physician and founder of Tandem Clinic, where she focuses on Lyme disease, chronic infection, and complex chronic illness using an integrative and systems-based clinical framework. As a Lyme Literate ND (LLND), she is trained in contemporary diagnostics and treatment strategies for challenging infectious and autoimmune presentations and has developed Canada’s first CNME-accredited naturopathic residency in vector-borne illness and chronic complex disease. Dr. Klassen is passionate about improving recognition and care for patients often overlooked by conventional systems and contributes to clinician education and training in chronic infection management.
 Dr. Ece Toprak, ND is a licensed naturopathic physician and graduate of the Canadian College of Naturopathic Medicine (CCNM), where she completed her foundational training in integrative medicine. Dr. Toprak is dedicated to evidence-informed clinical practice and has contributed to naturopathic research and presentations during her academic training, including student-faculty collaborations on clinical topics at CCNM. She brings a systems-based perspective to patient care, incorporating comprehensive assessment, lifestyle medicine, botanical and nutritional therapeutics, and individualized treatment planning to support complex and multisystem health concerns.
Dr. Ece Toprak, ND is a licensed naturopathic physician and graduate of the Canadian College of Naturopathic Medicine (CCNM), where she completed her foundational training in integrative medicine. Dr. Toprak is dedicated to evidence-informed clinical practice and has contributed to naturopathic research and presentations during her academic training, including student-faculty collaborations on clinical topics at CCNM. She brings a systems-based perspective to patient care, incorporating comprehensive assessment, lifestyle medicine, botanical and nutritional therapeutics, and individualized treatment planning to support complex and multisystem health concerns.
References
- American Academy of Pediatrics. Pediatric acute-onset neuropsychiatric syndrome (PANS): clinical report. Pediatrics. 2025;155(3):e2024070334. doi:10.1542/peds.2024-070334.
- Swedo S, Menendez CM, Cunningham MW. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) 2024 Jul 7 [Updated 2024 Sep 13]. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]. 2nd edition. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2022 Oct 8. Chapter 26. Available from: https://www.ncbi.nlm.nih.gov/books/NBK607260/
- Frankovich J, Swedo S, Murphy T, et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part II-Use of Immunomodulatory Therapies. J Child Adolesc Psychopharmacol. 2017;27(7):574-593. doi:10.1089/cap.2016.0148
- Vreeland A, Calaprice D, Or-Geva N, et al. Postinfectious Inflammation, Autoimmunity, and Obsessive-Compulsive Disorder: Sydenham Chorea, Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infection, and Pediatric Acute-Onset Neuropsychiatric Disorder. Dev Neurosci. 2023;45(6):361-374. doi:10.1159/000534261
- Gagliano A, Carta A, Tanca MG, Sotgiu S. Pediatric Acute-Onset Neuropsychiatric Syndrome: Current Perspectives. Neuropsychiatr Dis Treat. 2023;19:1221-1250. Published 2023 May 24. doi:10.2147/NDT.S362202
- Delaney S, Robveille C, Maggi RG, et al. Bartonella species bacteremia in association with adult psychosis. Front Psychiatry. 2024;15:1388442. Published 2024 Jun 7. doi:10.3389/fpsyt.2024.1388442
- McDuffee NS, Steinour M, Shah K. Neuropsychiatric Manifestation of Tick-Borne Disease and the Importance of Screening in Endemic Regions. Prim Care Companion CNS Disord. 2025;27(4):25cr03948. Published 2025 Aug 14. doi:10.4088/PCC.25cr03948
- Bransfield RC. The psychoimmunology of lyme/tick-borne diseases and its association with neuropsychiatric symptoms. Open Neurol J. 2012;6:88-93. doi:10.2174/1874205X01206010088
- Lins KA, Drummond MR, Velho PENF. Cutaneous manifestations of bartonellosis. An Bras Dermatol. 2019;94(5):594-602. doi:10.1016/j.abd.2019.09.024
- Breitschwerdt EB, Greenberg R, Maggi RG, Mozayeni BR, Lewis A, Bradley JM. Bartonella henselae Bloodstream Infection in a Boy With Pediatric Acute-Onset Neuropsychiatric Syndrome. J Cent Nerv Syst Dis. 2019;11:1179573519832014. Published 2019 Mar 18. doi:10.1177/1179573519832014
- Stewart Z, Korsapathy S, Frohlich F. Crowd-sourced investigation of a potential relationship between Bartonella-associated cutaneous lesions and neuropsychiatric symptoms. Front Psychiatry. 2023;14:1244121. Published 2023 Oct 24. doi:10.3389/fpsyt.2023.1244121
- Cross A. Case Report: PANDAS and persistent Lyme disease with neuropsychiatric symptoms: treatment, resolution, and recovery. Front Psychiatry. 2021;12:505941. doi:10.3389/fpsyt.2021.505941.
- Brown KD, Farmer C, Freeman GM Jr, et al. Effect of Early and Prophylactic Nonsteroidal Anti-Inflammatory Drugs on Flare Duration in Pediatric Acute-Onset Neuropsychiatric Syndrome: An Observational Study of Patients Followed by an Academic Community-Based Pediatric Acute-Onset Neuropsychiatric Syndrome Clinic. J Child Adolesc Psychopharmacol. 2017;27(7):619-628. doi:10.1089/cap.2016.0193
- Stancil SL, Abdel-Rahman S, Wagner J. Developmental Considerations for the Use of Naltrexone in Children and Adolescents. J Pediatr Pharmacol Ther. 2021;26(7):675-695. doi:10.5863/1551-6776-26.7.675
- Theriault C, et al. The efficacy of low-dose naltrexone in pediatric chronic pain: a retrospective analysis. J Pain. 2023;24(4):84-85.