JACOB SCHOR, ND, FABNO
In recent years, hypothermia – the lowering of body temperature for therapeutic purposes – has been adopted in neonatal intensive care facilities across the country for the treatment of hypoxia-induced encephalopathy in newborns. In simpler terms, this refers to brain damage from asphyxia, or suffocation, often brought about by the umbilical cord wrapping around the infant’s neck. While use of hypothermia for this particular condition is likely outside the scope of practice of naturopathic physicians, hypothermia itself is among the most fundamental and traditional naturopathic therapies for treating illness. There is value in our being cognizant of this treatment’s application in the neonatal realm. For those of us who in the course of practice may deal with hypoxic newborns, this article should be a timely reminder of the importance of having emergency referral systems in place and up to date. While hypothermia can be near-miraculous in helping newborns recover from brain injury, it only helps if started within the 6-hour window after birth. For the rest of us, knowing more about this specialized use of hypothermia may allow us to better understand the underlying mechanisms of action so that we may translate this application into other situations where hypoxia and reperfusion injuries occur.
We were exposed to the basic ideas of hypothermia when we studied hydrotherapy as naturopathic students. Water has a high heat capacity, so is often employed to raise or lower body temperature. However, in hydrotherapy we typically use cold water to trigger a reactive flow of blood to the cooled area in order to warm it. Hydrotherapy, of course, is far more complex than that. In an excellent 2014 article published here in NDNR,1 Sussanna Czeranko reviewed the distinctions between the goals of 4 forms of hydrotherapy: fluxion, reaction, retrostasis, and revulsion:
… fluxion speeds up the flow of blood, reaction initiates the body’s healing responses, retrostasis moves blood from the surface of the skin to the organs, and revulsion moves blood from one part to another distally.1
Neonatal Hypothermia
In this particular article, hypothermia of newborns is still achieved through cold water. However, in this instance, the goal is to reduce the body temperature and maintain that lower temperature such that it overrides compensatory attempts of the body to re-warm itself.
Hypothermia treatments are directed to cool either a specific area of the body or to systemically cool the entire body. Those of us who work with cancer patients are aware of the currently-in-vogue cooling caps used during chemotherapy to prevent or reduce hair loss. In that circumstance, the effect is directed only toward the scalp to prevent damage to the hair follicles. Hypothermia treatment of neonates can be either whole-body or directed to the head, and while recent reviews suggest possibly greater benefits from the latter,2 my impression is that whole-body cooling is currently the method used most often. Using what is essentially a crib-sized waterbed with tightly regulated water temperatures, the infant is cooled to a core temperature (measured as an esophageal temperature) of 33.5 °C (92.3 °F) for 72 hours.
While we might consider hydrotherapy a naturopathic discipline dating back to Priessnitz,3 this modern usage to cool the brain and treat hypoxic encephalopathy dates back only to the early 1980s, when case reports were published of children who survived cold-water drowning with negligible neurologic damage.4.5 Such reports led to animal experiments that, in turn, led to human trials.6 The first clinical trials examining babies were published in the late 1990s7 and early 2000s.8-11 In the years since, hypothermia has been studied repeatedly, to the degree that we now look to meta-analyses and Cochrane reviews to confirm benefit.12
A 2007 Cochrane review that included 8 randomized controlled trials (RCTs) concluded that “…therapeutic hypothermia treatment for term infants with moderate to severe HIE [hypoxia-induced encephalopathy] significantly reduced death as well as long-term neurodevelopmental disabilities to 18 months of age. Most importantly, therapeutic hypothermia improved mortality and neurodevelopmental outcomes among survivors.”13
A 2013 Cochrane review updated these findings.14 Analyzing 11 RCTs of term- and late-preterm infants with moderate/severe encephalopathy (n=1505), “Therapeutic hypothermia resulted in a statistically significant and clinically important reduction in the combined outcome of mortality or major neurodevelopmental disability to 18 months of age (typical RR [risk ratio]: 0.75) … Cooling also resulted in statistically significant reductions in mortality (typical RR: 0.75), …”14
In China, where hypothermia is not fully accepted, over half of the hospitals surveyed were found to have recently provided this treatment.15 A statistic summarizing the percentage of US hospitals possessing the necessary equipment to offer hypothermia remains elusive, but it seems that the number might be lower than in China: “Because the majority of infants who have neonatal encephalopathy are born at community hospitals, centers that perform cooling should work with their referring hospitals to implement education programs focused on increasing the awareness and identification of infants at risk for encephalopathy, and the initial clinical management of affected infants.”16 In the United States, infants are transported to tertiary hospitals with neonatal intensive care units (NICUs) for treatment. The American Academy of Pediatrics maintains an online search tool to locate the nearest NICUs to a specified location.17
Phases of Brain Injury
Understanding the mechanisms by which hypothermia helps these injured neonates may be useful for us, as it may add a dimension of understanding to how some naturopathic therapies work. Let’s focus first on brain injury in hypoxic infants. A cascade of brain injuries is triggered by a lack of oxygen. For ease of explanation, this cascade is often divided into 3 phases.18
In the acute phase of injury, “… the culmination of energy failure, acidosis, glutamate release, lipid peroxidation, and the toxic effect of nitric oxide leads to cell death via necrosis and activates apoptotic cascades.”19 During this phase, hypoxia causes a switch from oxidative to anaerobic metabolism. Inflammation, along with excitotoxicity from glutamate and intracellular calcium overload, promote cellular damage and activate apoptosis. The acute phase is followed by partial recovery and a latent phase of injury that lasts up to 6 hours. Some oxidative metabolism is restored during this phase; however, inflammation and apoptotic cascades continue.
Then secondary deterioration sets in. This secondary phase begins 6-15 hours after the initial injury and may last hours to days. Mitochondrial dysfunction and energy failure occur, along with continued cytotoxicity, which lead to further brain injury and cell death.20
The third phase involves processes that can occur months after the initial injury and include late cell death, remodeling of the brain, and “… astrogliosis due to persistent inflammation and epigenetic changes.”21 (Note: Astrogliosis is a defense mechanism that helps minimize and repair the damage after injury to the CNS).22 “It is the time period following resuscitation, before the secondary phase of injury, that provides a potential window for neuroprotection or diminution of injury.”21 In other words, this is where hypothermia can come into play, during the second stage where damage continues to accumulate even though oxygenation has been restored.
Naturopathic Adjuncts?
Hypothermia is currently so well accepted as the primary treatment for hypoxic encephalopathy that much of the current research is focused instead on adjunctive therapies that might make hypothermia more effective.23 Examples include xenon or hydrogen inhalation,24,25 melatonin,26 cannabidiol (CBD),27 erythropoietin,28 and carnosine.29 A number of natural products are being considered as prophylactic agents to administer during pregnancy, as they might offer protection to the fetus and neonate. These include polyphenols, omega-3 fatty acids, vitamins, plant-derived compounds (tanshinones, sulforaphane, and capsaicin), and endogenous compounds (melatonin, carnitine, creatine, and lactate).30 These agents all seem to share anti-inflammatory, anti-oxidative, anti-apoptotic, and neurofunctional regulatory properties.23
Also, animal data theoretically suggest additional plant extracts that might be protective in human newborns, including pomegranate,31 grape seed extract,32 quercetin,33 saffron,34 and Salvia miltiorrhizae.35
It is conceivable that an expectant mother could be encouraged to drink pomegranate juice days or weeks prior to delivery. Yet it is difficult to imagine women, even those at high risk for birth complications, making the effort to take nutritional supplements just in case they might help.
Some combination of these herbal extracts could be helpful for those more proactive patients; however, mothers should be understandably hesitant until strong human evidence supports their use.
Other Uses of Hypothermia
In recent years, neonatal specialists have begun prescribing hypothermia treatment more liberally and treating children outside of the initial criteria that signal severe brain injury. Studies are now assessing the application of hypothermia to milder cases. At this point, questions remain as to whether this is justified.
Recent studies have also expanded the list of other possible uses of hypothermia. A February 2021 meta-analysis evaluated data on kidney function, as acute kidney injury is a frequent complication of perinatal asphyxia.36 The authors reported a 19% reduction in acute kidney injury in infants treated with hypothermia (RR: 0.81) Additionally, 4 out of 5 identified studies reported significant reductions in cardiac biomarkers as well as less myocardial dysfunction on ECG and cardiac ultrasound.36
Use of the modality has expanded beyond newborns and children:
Hypothermia is widely accepted as the gold-standard method by which the body can protect the brain. Therapeutic cooling—or targeted temperature management (TTM)—is increasingly being used to prevent secondary brain injury in patients admitted to the emergency department and intensive care unit. Rapid cooling to 33 °C for 24 h is considered the standard of care for minimizing neurological injury after cardiac arrest….37
Knowing how hypothermia reduces hypoxic brain injury in neonates may help us better understand its use in other conditions and patient cohorts. A technique of inducing hypothermia was developed by Bigelow and used as early as 1949 to stop the heart’s circulation for 15 minutes while open-heart surgery was performed.38,39 Similar techniques have been used and further refined in intervening years. As the authors of a 2011 review wrote, “Within the past decade, the efficacy of hypothermia to treat emergency cases of ongoing ischemia such as stroke, myocardial infarction, and cardiac arrest has been studied. Although the exact role of ischemia/reperfusion is unclear clinically, hypothermia holds significant promise for improving outcomes for patients suffering from reperfusion after ischemia.”40
The idea that hypothermia is useful for treating neonatal brain injury resulting from anaerobic metabolism and for preventing resultant mitochondrial failure may inspire us to consider other conditions where anaerobic metabolism leads to injury. We already use cold in the form of ice for post-exercise muscle pain and injury.
What about with cancer? Many of us talk about how cancer cells switch to anaerobic respiration. Could cold therefore be employed against cancer? We tend to think first of hyperthermia as a cancer treatment, but could hypothermia also be useful? There are recent indications that this indeed may be the case. A March 2021 report described how hypothermia restored function to mutated p53 enzymes, a major promoter of cancer cell death.41 Then in May 2021, an in-vitro study reported that cooling glioblastoma tumors significantly enhanced standard treatments.41
Research findings on therapeutic hypothermia, however, are far from unanimous. One recent clinical trial published in May 2021, subjected 58 adult patients to hypothermia immediately after standard interventions for myocardial infarct and compared them to 53 control patients.42 The results were not all that positive-sounding: “Major adverse cardiac events at 30 days increased non-significantly in the hypothermia group (8.6% vs 1.9%; p=0.117) while cardiogenic shock (10.3% vs 0%; p=0.028) and paroxysmal atrial fibrillation (43.1% vs 3.8%; p=0.001) were significantly more frequent in the hypothermia group.” Problems with the study design may explain the worse outcome in the hypothermia group to some extent. Still, these findings aren’t what we would have hoped to see.42
Closing Thoughts
Our patients are not average people. Often, they come to see us in part because they have unusual health responses. Their health conditions may make their lives more challenging, or they may hold world views that lie on the fringes of normal. We need to be prepared for the unexpected. If your practice includes neonates, you need to know which hospitals in your area offer hypothermia, and have their phone numbers handy. Many NICUs dispatch specially equipped ambulances so that cooling can be started while the infant is being transported to the hospital.
This discussion has mostly been about neonates, not preterm babies. Infants that emerge from the womb too early often suffer from frank hypothermia. This is a life-threatening situation, and preterm infants need to be kept warm.43 Being able to distinguish between infants who need to be warmed and those that should be cooled is a skill-set we won’t attempt to teach here. What you need to learn is the phone number of a NICU to reach out to when help is needed.
In the end we may fall back on alternating heat and cold. For the moment, though, hypothermia is an avenue of therapy we should be keeping our eyes on.
References:
- Czeranko S. Hydrotherapy Terms Defined: Fluxions, Reactions, Retrostasis, and Revulsions. NDNR. 2014;10(9):22-25. Available at: https://ndnr.com/nature-cure/hydrotherapy-terms-defined-fluxions-reactions-retrostasis-and-revulsions/. Accessed October 10, 2021.
- Assis FR, Narasimhan B, Ziai W, Tandri H. From systemic to selective brain cooling – Methods in review. Brain Circ. 2019;5(4):179-186.
- Czeranko S. Vincent Priessnitz (1799-1851). Integr Med (Encinitas). 2019;18(4):25.
- Young RS, Zalneraitis EL, Dooling EC. Neurological outcome in cold water drowning. JAMA. 1980;244(11):1233-1235.
- Sekar TS, MacDonnell KF, Namsirikul P, Herman RS. Survival after prolonged submersion in cold water without neurologic sequelae. Report of two cases. Arch Intern Med. 1980;140(6):775-779.
- Young RS, Olenginski TP, Yagel SK, Towfighi J. The effect of graded hypothermia on hypoxic-ischemic brain damage: a neuropathologic study in the neonatal rat. Stroke. 1983;14(6):929-934.
- Gunn AJ, Gluckman PD, Gunn TR. Selective head cooling in newborn infants after perinatal asphyxia: a safety study. Pediatrics. 1998;102(4 Pt 1):885-892.
- Battin MR, Dezoete JA, Gunn TR, et al. Neurodevelopmental outcome of infants treated with head cooling and mild hypothermia after perinatal asphyxia. Pediatrics. 2001;107(3):480-484.
- Zupan V. Systemic hypothermia in infants with hypoxic-ischaemic encephalopathy: a French pilot study. Dev Med Child Neurol Suppl. 2001;86:32.
- Debillon T, Daoud P, Durand P, et al. Whole-body cooling after perinatal asphyxia: a pilot study in term neonates. Dev Med Child Neurol. 2003;45(1):17-23.
- Battin MR, Penrice J, Gunn TR, Gunn AJ. Treatment of term infants with head cooling and mild systemic hypothermia (35.0 degrees C and 34.5 degrees C) after perinatal asphyxia. Pediatrics. 2003;111(2):244-251.
- Young RS, Olenginski TP, Yagel SK, Towfighi J. The effect of graded hypothermia on hypoxic-ischemic brain damage: a neuropathologic study in the neonatal rat. Stroke. 1983;14(6):929-934.
- Jacobs S, Hunt R, Tarnow-Mordi W, et al. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2007;(4):CD003311.
- Jacobs SE, Berg M, Hunt R, et al. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2013;2013(1):CD003311.
- Wang Z, Zhang P, Zhou W, et al. Neonatal hypoxic-ischemic encephalopathy diagnosis and treatment: a National Survey in China. BMC Pediatr. 2021;21(1):261.
- Committee on Fetus and Newborn. Hypothermia and Neonatal Encephalopathy. Pediatrics. 2014;133(6):1146-1150.
- American Academy of Pediatrics. [Home page]. Available at: https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/nicuverification/Pages/NICUSearch.aspx. Accessed October 10, 2021.
- Hassell KJ, Ezzati M, Alonso‐Alconada D, et al. New horizons for newborn brain protection: enhancing endogenous neuroprotection. Arch Dis Child Fetal Neonatal Ed. 2015;100(6):F541‐F552.
- Ferriero DM. Neonatal brain injury. New Engl J Med. 2004;351(19):1985‐1995.
- Douglas‐Escobar M, Weiss MD. Hypoxic‐ischaemic encephalopathy: a review for the clinician. JAMA Pediatr. 2015;169(4):397‐403. Available at: https://www.perinatal.com.br/simposio2016/pdf/aula04-asfixia-review.pdf. Accessed October 11, 2021.
- Fleiss B, Gressens P. Tertiary mechanisms of brain damage: a new hope for treatment of cerebral palsy? Lancet Neurol. 2012;11(6):556‐566.
- Sharma K, Zhang G, Li S. Chapter 11 – Astrogliosis and Axonal Regeneration. Regeneration (Oxford). 2015:181-196. https://www.sciencedirect.com/science/article/pii/B9780128017326000112. Accessed October 11, 2021.
- Mohsenpour H, Pesce M, Patruno A, et al. A Review of Plant Extracts and Plant-Derived Natural Compounds in the Prevention/Treatment of Neonatal Hypoxic-Ischemic Brain Injury. Int J Mol Sci. 2021;22(2):833.
- Rüegger CM, Davis PG, Cheong JL. Xenon as an adjuvant to therapeutic hypothermia in near-term and term newborns with hypoxic-ischaemic encephalopathy. Cochrane Database Syst Rev. 2018;8(8):CD012753.
- Domoki F. Hydrogen-induced Neuroprotection in Neonatal Hypoxic-ischemic Encephalopathy. Curr Pharm Des. 2021;27(5):687-694.
- Pang R, Advic-Belltheus A, Meehan C, et al. Melatonin for Neonatal Encephalopathy: From Bench to Bedside. Int J Mol Sci. 2021;22(11):5481.
- Martínez-Orgado J, Villa M, Del Pozo A. Cannabidiol for the Treatment of Neonatal Hypoxic-Ischemic Brain Injury. Front Pharmacol. 2021;11:584533.
- Yang G, Xue Z, Zhao Y. Efficacy of erythropoietin alone in treatment of neonates with hypoxic-ischemic encephalopathy: A protocol for systematic review and meta-analysis. Medicine (Baltimore). 2021;100(24):e26365.
- Byun JC, Lee SR, Kim CS. Effects of carnosine and hypothermia combination therapy on hypoxic-ischemic brain injury in neonatal rats. Clin Exp Pediatr. 2021;64(8):422-428.
- Reyes-Corral M, Sola-Idígora N, de la Puerta R, et al. Nutraceuticals in the Prevention of Neonatal Hypoxia-Ischemia: A Comprehensive Review of their Neuroprotective Properties, Mechanisms of Action and Future Directions. Int J Mol Sci. 2021;22(5):2524.
- Ahmed MA, El Morsy EM, Ahmed AA. Pomegranate extract protects against cerebral ischemia/reperfusion injury and preserves brain DNA integrity in rats. Life Sci. 2014;110(2):61-69.
- Feng Y, Liu YM, Fratkins JD, LeBlanc MH. Grape seed extract suppresses lipid peroxidation and reduces hypoxic ischemic brain injury in neonatal rats. Brain Res Bull. 2005;66(2):120-127.
- Wu M, Liu F, Guo Q. Quercetin attenuates hypoxia-ischemia induced brain injury in neonatal rats by inhibiting TLR4/NF-κB signaling pathway. Int Immunopharmacol. 2019;74:105704.
- Huang A, Jia L. Crocin enhances hypothermia therapy in hypoxic ischemia-induced brain injury in mice. Acta Neurol Belg. 2021;121(2):429-436.
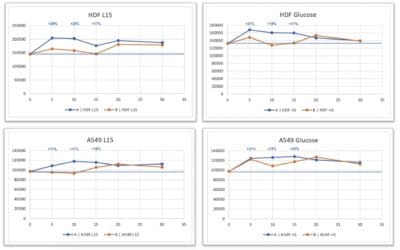
- Li MY, Zhang YB, Zuo H, et al. Protective effect of pretreatment of Salvia miltiorrhiza Bunge. f. alba plasma against oxygen-glucose deprivation-induced injury of cultured rat hippocampal neurons by inhibiting apoptosis. Sheng Li Xue Bao. 2012;64(1):41-47. [Article in Chinese]
- van Wincoop M, de Bijl-Marcus K, Lilien M, et al. Effect of therapeutic hypothermia on renal and myocardial function in asphyxiated (near) term neonates: A systematic review and meta-analysis. PLoS One. 2021;16(2):e0247403.
- Choi HA, Badjatia N, Mayer SA. Hypothermia for acute brain injury–mechanisms and practical aspects. Nat Rev Neurol. 2012;8(4):214-222.
- Presciutti A, Perman SM. The evolution of hypothermia for neuroprotection after cardiac arrest: a history in the making. Ann N Y Acad Sci. 2021 Sep 23. doi: 10.1111/nyas.14676.
- Olin C. The first open heart surgery–a cool story. Winter sleep of marmosets inspired the breakthrough. Lakartidningen. 2002;99(45):4498-4499. [Article in Swedish]
- Lampe JW, Becker LB. State of the art in therapeutic hypothermia. Annu Rev Med. 2011;62:79-93.
- Fulbert C, Chabardès S, Ratel D. Adjuvant therapeutic potential of moderate hypothermia for glioblastoma. J Neurooncol. 2021;152(3):467-482.
- Noc M, Laanmets P, Neskovic AN, et al. A multicentre, prospective, randomised controlled trial to assess the safety and effectiveness of cooling as an adjunctive therapy to percutaneous intervention in patients with acute myocardial infarction: the COOL AMI EU Pivotal Trial. EuroIntervention. 2021;17(6):466-473.
- Mank A, van Zanten HA, Meyer MP, et al. Hypothermia in Preterm Infants in the First Hours after Birth: Occurrence, Course and Risk Factors. PLoS One. 2016;11(11):e0164817.
Jacob Schor, ND, FABNO graduated from NCNM in 1991 and has practiced in Denver, CO, ever since. He has been active in state association politics, taking his turn as president of the Colorado Association of Naturopathic Doctors and Legislative Chair. Dr Schor has also held leadership positions in the Oncology Association of Naturopathic Physicians, served on the AANP Board of Directors, and chaired the AANP’s speaker selection committee. For the past decade he has been the Associate Editor of the Natural Medicine Journal, and is a regular contributor to the Townsend Letter.