")
An evidence-informed, dysfunction-based approach to evaluating spike protein effects, comorbidities, coagulation abnormalities, immune dysregulation, and mitochondrial dysfunction.
Paul S. Anderson, NMD
Abstract
This clinical update summarizes a structured framework for assessing and managing Long COVID and post-vaccination syndromes using spike antibody monitoring, comorbidity stratification, and the Klok functional status scale. It outlines tiered laboratory evaluation and integrative therapeutic strategies targeting coagulation, immune modulation, mitochondrial dysfunction, detoxification, and systemic inflammation.
INTRODUCTION:
Addressing people with Long-COVID (LC) and Vaccine Injuries/Post-Vaccination effects (PV) are two increasing clinical priorities in current medical practice.
In September 2025, NDNR published my review of this topic https://ndnr.com/long-covid-vaccine-injuries-treatment/ as “Post-Pandemic Clinical Medicine: Addressing Long-COVID and Vaccine Injuries”. This clinical summary is directly tied to that publication as the majority of the scientific citations and detail are contained in it.
The purpose of this summary is to “boil down” the assessment and treatment flow set forth in the original publication.
NOTE: All references are found in the original publication, unless specified in the text below.
ASSESSMENT AND INITIAL INTERVENTIONS:
For either LC or PV assessment there are two broad methods of assessment, those being direct trigger assessment (Spike-protein, cytokines etc.) and whole-case comorbidity assessment. Both will be outlined below.
First obtain a baseline spike antibody level.
1: BASELINE: Spike Protein / Cytokine Assessment:
- SARS-CoV-2 Semi-Quantitative Total Antibody, Spike [S-Protein, Semi-quant]
- SARS-CoV-2 Antibodies, Nucleocapsid [N-Protein, Qualitative]
Recall from the original paper that the “N” protein is a marker of COVID infection and may be helpful in differentiating infection-triggered versus vaccine-triggered spike levels.
As outlined in the original paper, the level of “S” protein differs between CV and PV presentations.
- COVID infection triggers “S” rises to 500–800 U/mL and begins to fall after 90 days.
- Vaccine induced “S” can be 800–1000 to over 25,000 U/mL and has been noted in the data at 245 days.
Direct “SPIKE” Testing?
Direct “spike” testing is not available at the time of publication in the US, but in the original publication I list a source in Europe which can detect S-Protein, Modified mRNA, and Plasmid-DNA.
Indirect Inflammatory Mediator Testing?
Some labs (referenced in the original publication) test individual cytokines using data regarding cytokine-based pathophysiology of Long COVID symptoms that may include Il-1 series, IL-2, IL-4, IL-6, IL-10, TNF-α, IFN-g, and IL-17A.
Other publications recommend the following markers: Il 2, 4, 6, 8, 10, 13 GM-CSF, IFN-g, VEGF, (s)CD40l, CCL.
2: COMORBIDITY ASSESSMENT – Dysfunction Based Assessment and Treatment:
To assess the level of dysfunction experienced by the patient with LC or PV, a grading system should be employed. This allows the clinician to stratify their diagnostic and therapeutic approach while prioritizing appropriate labs and other interventions.
Does it matter if one is assessing and treating PV or LC? In many senses, no. As the conditions are often overlapping, and both have influences from comorbid conditions beyond COVID or Spike protein, the approach to assessment and therapeutics can begin in the same place and be personalized as required. Multiple papers outline the comorbidities of LC and PV syndromes. These include endocrine deregulation, co-infections, coagulopathies, de-novo and aggravated autoimmunity, increased sensitivity to environmental toxicants, potential for oncogenic processes, and many others.
The simplest and most clinically useful scale for either LC or PV I have found was published by Klok et. al. In the discussion of assessments below. I will use this scale to stratify the clinical work-up details.
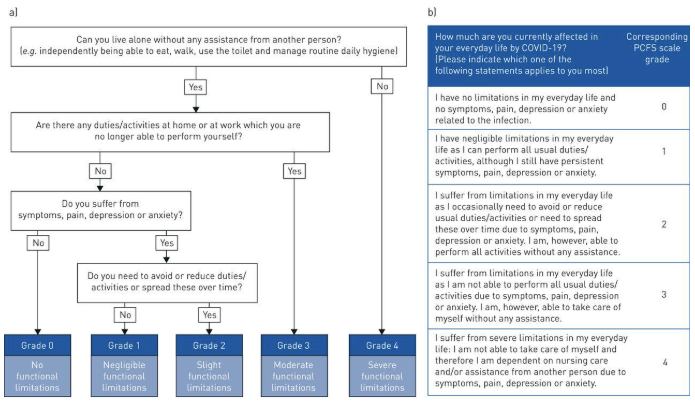
Graphic Below from: “Klok FA, Boon GJAM, Barco S, et al. The Post-COVID-19 Functional Status scale: a tool to measure functional status over time after COVID-19. Eur Respir J 2020; 56: 2001494”
A: Initial History: LC or PV
- Current Sn/Sx and effects on ADL (see the “Klok” scale above)
- Past History (active or inactive):
- CFS, FMS or other unexplained fatigue states
- Chronic Infections, Inflammatory (PANS, CIRS…)
- Autoimmunity or other Chronic Illness
- Chronic GI disease / syndromes
- Cancer
- Pain syndromes, migraine etc.
- Treatment for toxicity (mold, chemical, metal)
- Use of immunosuppressive therapies
- Clotting Disorders
- Neuropsychiatric History
- Any other relevant pre-existing condition
- COVID Vaccine, type and number
Assessment Targets: LC or PV
- Past History: Pertinent Positive Findings
- Mitochondrial Damage
- Blood-Brain Barrier (BBB – Neuroinflammation
- Clotting
- Inflammation
- Endocrine Dysregulation
- Infectious Agents & Resistance Factors
- GI Dysregulation
- Toxins
- Genomics
- Hallmarks, signs, or indications of occult or a known progressing cancer.
B: Clinical Dysfunction Based Assessment and treatment Ideas
Klok Asymptomatic Grade – 0
- Monitor basic labs: CBC, Ferritin, CMP-14, CRP, D-dimer, AlkPhos, LDH, CPK
- As a baseline: SARS-CoV-2 Semi-Quantitative Total Antibody, Spike [S-Protein, Semi-quant]
- If assessing presence of antibodies from infection: SARS-CoV-2 Antibodies, Nucleocapsid [N-Protein, Qualitative]
- Monitor any pre-existing abnormal labs (i.e. HbA1C, Thyroid…)
- Rx: Exercise, Low Inflammation Diet, Centering/Meditation, Hydration
- Consider empiric anticoagulant therapies as clinically indicated:
- Nattokinase, low dose 2000–3000 fibrinolytic units per day, on an empty stomach (or other enzyme therapies).
- Vitamin E 200–400 IU daily
- Inclusion of anticoagulant support is proposed based on prior papers cited in the original publication as well as the new data published by Thierry, et.al.1
- Implement or keep them on the basic nutritional interventions:
- Vit. A, D/K2, E; Vit. C, B-Complex, Multimineral …
- Treat acute issues PRN
- Taper to baseline supplements in 2-3 months
- Have them contact you if the situation changes.
Klok Mild Grade 1 – 2
- The above listed “Klok Grade-0” labs and assessments plus:
-
- Re-test any pre-existing conditions
- Increase coagulopathy assessment to include D-dimer (quantitative), Fibrinogen activity, Platelet Count, PT-INR
- Expanded Thrombosis and Venous Risk Profiles may be necessary in more advanced cases and can include:
- Anticardiolipin antibodies, IgG and IgM
- Antithrombin activity
- β2-glycoprotein 1 antibodies, IgA, IgG, and IgM
- D-dimer
- dRVVT screen
- Factor II
- (prothrombin) mutation analysis
- Factor V Leiden mutation analysis
- Protein C, functional
- Protein S antigen, free
- Expanded Thrombosis and Venous Risk Profiles may be necessary in more advanced cases and can include:
- Calculate Neutrophil/Lymphocyte ratio and follow as a serial marker (higher NLR = worse inflammation).73
- Add: RBC Mineral Profile or at least RBC Zn, Cu, Mg
- Add: GGT; ANA with Reflex
- Endo: rT3/Ft3/4, Thyroid Ab’s, TSH / AM Cortisol / Consider Estrogen / Progesterone / Testosterone
- ID: ASO, Chlamydia and Mycoplasma pneumoniae., Candida, EBV, Total Ig-G/M/A/E (others as clinically indicated – especially if prior positive.)
- Unchallenged Urine Toxic Metals (UTM) (norm values to NHANES)74, Consider Mycotoxin and Chemical toxin screening
- Empiric therapies:
- Treat any abnormalities found on initial labs.
- Anticoagulant therapies:
- Nattokinase, low dose 4000–6000 fibrinolytic units per day on an empty stomach (or other enzyme therapies).
- Vitamin E 200–400 IU daily
- Others as clinically indicated
- Neurosteroids (low first-pass progesterone or pregnenolone). Use of micronized preparations in oil, sublingual drops or tablets, or troches. Doses of 100 to 200 mg nightly are common.
- Immune-balancing:
- Balance 25 (OH) and 1,25 (OH) Vitamin D3 levels
- Assure Vitamin D supplementation is balanced with Vitamin K2
- Immune focused mushroom therapies if indicated
- Low Dose Naltrexone
- Ivermectin 0.2 to 0.4 mg / kg [see notes in original paper.]
- Monitor q-2-4 weeks in follow up
Klok Moderate Grade – 3
- All the above listed labs and assessment in “Klok Grade 0, 1, 2” plus:
-
- Aggressively treat Endo / ID / Toxic and other cause areas.
- Add on:
- Other infectious screening: Lyme and Coinfections, Other Viruses, GI Testing for all infections
- OAT (Organic Acids Test)
- Post challenge UTM (you already have a “pre” from above), Mycotoxin and Chemical Toxin screening
- Add on, if not already included:
- Neurosteroid therapy and neuro repair / immunomodulatory immunotherapies, as noted above
- LDN Rx.
- Phase-2 Biofilm Rx.
- HBOT if they can gain access, either HBOT level will work:
- 1.3 – 1.5 ATA 60-90 min with 3-4L O2
- or 2.0 – 2.75 ATA with O2 by mask 15L (may need air-break mid therapy) 2-5X a week initially.
- Any COVID or Post-COVID patient would benefit from HBOT
- Other Rx. as indicated
- Consider mitochondrial therapies as needed such as NAD, Methylene Blue, Red / Near IR Light Therapy, etc.
- Monitor closely.
Klok Severe Grade – 4
- In my (and others) experience you cannot “phase in” these peoples work up.
- A very critical look at any past illness or syndrome and follow-up is required.
- All areas listed for Endo, Tox, ID etc. must be assessed and aggressively treated.
- The longer they have had LC or PV Sn/Sx and the more past / comorbidities, the longer needed to treat. But they will get better if you are aggressive.
C: Additional Therapies:
The above disfunction based strategies are the best place to start as far as assessment and basic treatment are concerned. All numeric references noted below are found in the original publication.
For both LC and PV the following areas are critical to consider:
- Identify, Treat, and Support Comorbidities
- Support Clotting / Coagulation Issues
- Block Spike-protein from entering cells
- Degrade Spike-protein
- Modulate Immune Function
- Support Antioxidant and Nutrient Status
- Support Mitochondrial Function
Below are some therapeutic ideas which have repeatedly shown positive outcomes across a large provider group. This is not an exhaustive list but rather interventions which have high therapeutic yield.
1.Identify, Treat, and Support Comorbidities
The above section denoting the use of the “Klok” scale and assessment and therapeutic ideas covers this area well.
Please note: If the comorbidities are not addressed the therapeutics that follow will have partial or temporary effect at best. The therapeutics below assume underlying conditions and comorbidities are being addressed.
2. Support Clotting / Coagulation Issues
Coagulopathies are ubiquitous in LC and PV. Treatment ranges from therapies for obvious coagulopathy to empiric treatment for micro clotting. The focus therapeutically in the prescription realm is factor Xa drugs, heparin therapy, aspirin, clopidogrel, curcumin, and others. In the natural therapy realm, enzymes, essential fatty acids, vitamin E and others are common.
A common clinical question is “can people on factor Xa drugs, heparin therapy, aspirin, clopidogrel, or a combination of these use any natural anticoagulants?” The answer is generally yes, because the natural agents below work in different parts of the clotting cascade.
These are the following interventions commonly used:
- Enzyme therapy is used in all patients. [I will use Nattokinase as an example but Lumbrokinase or Serratiopeptidase (also known as serrapeptase) can work as well. Also note that Lumbrokinase may have more effect if thrombi have already formed.] 112, 113
- Nattokinase baseline dose is 2000 Units in the AM before eating
- Nattokinase in higher risk people can be dosed between 4000 and 10,000 Units daily.
- Vitamin E as mixed tocopherols 200 to 400 IU daily
- Omega-3 1000 to 2000 mg total Omega-3 daily 114 – 116
- Curcumin is a week anticoagulant but an excellent tissue protectant. If it clinically is appropriate. 102 – 104
- Different forms of curcumin have different dose strategies. I use Curcumin phytosome at 500 to 1000 mg per day
- In high-risk people I will add 81 mg Aspirin daily (if they are not on it). 134
3. Bind Spike-protein and or Block from entering cells
Ivermectin 84 – 88, as well as quercetin 40, 107 – 111, curcumin 102 – 104, rutin 105, dandelion leaf 135, milk thistle 106, and Andrographis 136 – 138 are studied for this.
My practice has been to use Ivermectin at 0.2 to 0.4 mg / kg (rounded to the nearest even number for prescribing ease) given in one dose at night, as it can have some GABA / somnolent effect. I dose this daily for two to four months as a base therapy and then see how they do if I stop the dose. If they aggravate when discontinuing the Ivermectin then they can return to the daily dose. It can be dosed long term until the person has clinical remission. Safety note: I have used Ivermectin in cancer patients for over twenty years and it is incredibly safe if used long term.
I will generally add one more natural agent. If they are on curcumin that is a good synergist. I typically add milk thistle 500 – 800 mg with dinner for this purpose but also to help as a liver support as well. If “pill count overload” is an issue then curcumin can fill that dual role.
Additionally the flavonoid Rutin has some data on Spike-protein binding.105
4. Degrade Spike-protein
Nattokinase is a subtilisin-like alkaline serine protease which has been shown to not only be anticoagulant 112 but also degrade the Spike-protein 113. Other enzymes in this class likely have similar effects but nattokinase is the one currently with positive data. The above mentioned dosing for anticoagulation can be sufficient. In sick individuals with high Spike antibodies I will generally assure the dose of nattokinase is 4000 – 10,000 Units daily away from food for the first three or more months.
There is a current discussion of the possibility of enzyme therapies aggravating these cases due to “incomplete breakdown” of the Spike-protein. While this theory sounds intriguing if one looks at the data on how completely nattokinase breaks down Spike-protein it would appear this fear is unfounded.
Depuration and Detoxification
Depuration (whole body supported elimination) and detoxification (specific pathway support) obviously go hand in hand. The process of LC or PV illness treatment will either directly or indirectly have these factors involved.
If a comorbidity of a toxin / toxicant presence is found then whatever specific therapies used for that comorbidity may be enough to assist. With or without direct toxin / toxicant treatment every person dealing with LC or PV has a need for some level of depuration and detoxification.
Options (as clinically indicated) include:
- Body movement and hydration
- Heat therapies
- Hydrotherapy of many types
- High fiber foods and or binder type supplements
- Nutrient and antioxidant support
- Specific therapies (chelation, oxidation, etc.)
- Blood filtration therapies:
- Apheresis – Plasmapheresis / Therapeutic Plasma Exchange
- Extra-corporeal Blood Ozonation and Oxygenation (EBOO)
- Plasma donation
- Blood donation
5. Modulate Immune Function
Both LC and PV are hallmarked by widespread immune deregulation. Some level of immune modulation support is necessary as treatment progresses. If comorbid infections exist then this may be a longer process. Many agents already mentioned above have immunomodulatory activity (such as curcumin, Ivermectin, milk thistle, etc.) but some additions I have seen helpful are:
- Low Dose Naltrexone (LDN) dosed as in autoimmune cases 93-97
- Acute H-1 and H-2 blockers (MCAS comorbidity) 89 – 91
- Colchicine 0.5 or 0.6 mg BID for widespread inflammation, especially if vascular or cardiac comorbidity exists. 97 – 99
- Melatonin. 101 Melatonin has the effect of circadian support at lower doses (1 – 10 mg) and also can act as a mitochondrial redox support at higher (20 + mg) doses as well.
- A combination acutely of Licorice 60 mg and Boswellia 200 mg given twice a day for fourteen days was also helpful. 125
- Individually Licorice 120 – 124 and Boswellia 127 have data as well.
- Optimizing Vitamin D levels
- Other studied agents include:
- Quercetin 40, 107 – 111
- Luteolin 117 – 119
- Rutin 105
- Probiotics 131 – 134
- And Cinnamon, Clove, Ginger, Garlic, Thyme, Cardamom 139
6. Support Antioxidant and Nutrient Status
I will not elaborate greatly on the need for support of basic nutrition and antioxidant levels in the LC and PV patient. It is well documented in 139 and other resources for anyone needing a reference. There is an excessive use of glutathione and vitamin C as water soluble antioxidants in all chronic illness that should be addressed as the case progresses.
7. Support Mitochondrial Function
Clinicians generally have their favorite “go to” mitochondrial supports already in use. If this area is not addressed in the patient with LC or PV the case will typically progress slowly, and patient quality of life will be low.
Always assure that the basic factors which normally support the mitochondria and their function are in place. Dietary and supplemental amino acids, trace minerals, iron, b-vitamins, and other basic nutrients are crucial.
Acutely the following have been useful in recovering energy and also supporting other healing pathways. These should be used within their typical clinical guidelines for dose and safety. A short, but commonly helpful, list is:
- ALA, Co-Q10, and other “mitochondrial support” combinations
- NAD Support which can include IV NAD or NR, oral Niacinamide, and NR / NMN.
- Fasting 130
- Methylene Blue oral and or IV
- Red – Near IR Photodynamic Therapy
- FIR Sauna
- PEMF
- Hyperbaric Oxygen Therapy
Healing Expectations:
In my experience, it is similar to most complex chronic illness as far as the length of time and complexity of care required. These cases of LC and PV can be some of the most difficult a provider will see. It does help both the clinician and patient to have a baseline “grading” using the Klok scale as this can guide intensity of assessment and therapies as well as prognosticating the healing trajectory.
Estimated time to work on healing are:
- Klok – 0:
This is more of a monitoring and prevention stage. If one finds a comorbidity on initial testing then that may extend the time, but generally this is an initial assessment, basic interventions and follow up as required.
- Klok 1 & 2:
Depending on the comorbidities found these cases can start to see some progress in weeks to months. Generally, progress may wax and wane but will be on an upward trajectory. Some patients feel remarkably improved in six months and some in two years. As for following laboratory values use typical follow up intervals and let the patient know why you repeat some labs more or less frequently.
- Klok 3 & 4:
These patients typically have multiple comorbidities and require long term care and attention. Some features may clear moderately quickly (an example being a thyroid condition found upon initial assessment). Other features, especially aggravated or new autoimmunity, toxicity, etc. may be very long term issues. In many cases these long term issues are more chronic management items with the goal to improve overall function and quality of life rather than achieving a “full cure”.
- Note regarding using the Spike Antibody as baseline mentioned above: I generally do not test that more frequently than every six months. Symptomatic improvement is more critical than Spike Antibody drop. One correlation however to persistently elevated Spike Antibodies is the need to continue the Spike blocking, degrading, and anticoagulation therapies (as noted above) regardless of symptom improvement.
Factors which delay healing trajectory:
- Things that “didn’t look like they needed to be checked”:
- Some common ones include rT3, Cortisol, reproductive hormones, toxin-toxicants including chemical, metal and mycotoxins. Autoimmunity and Infections, especially if not present prior.
- Not re-checking and adjusting acute use therapies:
- Endocrine, GI, Infectious, Toxic, etc.
- Generally, not following up on and treating pertinent positives from old labs or new findings.
- Not appreciating the impact of long-term production of Spike from the mRNA vaccines, or the impact of COVID reinfection.
 Paul S. Anderson, NMD, is a licensed naturopathic physician with over three decades of clinical experience in complex chronic illness, infectious disease, immune dysregulation, and integrative oncology. A graduate of the National University of Natural Medicine (NUNM), Dr. Anderson has served as a medical director and educator across multiple institutions and is widely recognized for his expertise in combining conventional and naturopathic therapeutics in medically complex patients.
Paul S. Anderson, NMD, is a licensed naturopathic physician with over three decades of clinical experience in complex chronic illness, infectious disease, immune dysregulation, and integrative oncology. A graduate of the National University of Natural Medicine (NUNM), Dr. Anderson has served as a medical director and educator across multiple institutions and is widely recognized for his expertise in combining conventional and naturopathic therapeutics in medically complex patients.
He is the founder of Anderson Medical Specialty Associates and a frequent international lecturer on topics including chronic infections, IV therapeutics, environmental medicine, mitochondrial dysfunction, and advanced case management. Dr. Anderson has authored numerous educational programs and publications for healthcare professionals and is known for translating emerging research into structured, clinically actionable protocols that emphasize patient safety and systems-based care.
Original References can be found here: https://ndnr.com/long-covid-vaccine-injuries-treatment/
Additional References for this paper:
- Thierry AR, Usher T, Sanchez C, Turner S, Venter C, Pastor B, Waters M, Thompson A, Mirandola A, Pisareva E, Prevostel C, Laubscher GJ, Kell DB, Pretorius E. Circulating Microclots Are Structurally Associated With Neutrophil Extracellular Traps and Their Amounts Are Elevated in Long COVID Patients. J Med Virol. 2025 Oct;97(10):e70613. doi: 10.1002/jmv.70613. PMID: 41036702; PMCID: PMC12489976.

")