
Jared M. Skowron, ND
Brian was three-years old when I first saw him. One of the cutest little boys you ever saw, the pale face of atopy, the look of innocence, and a desire to sing and dance to impress the female office staff. They all would laugh at his rendition of Britney Spears, “Womanizer”. Brian’s mother was about to deliver her second boy, and flustered and at wit’s end: a single mother, pregnant, and chasing around a 3 year old.
The problem was that Brian would cry every time he tried to dance. Early in life, he was diagnosed with juvenile rheumatoid arthritis (JRA). His right knee was swollen and erythematous to the size of a blood-red orange. His lateral toes as well were inflamed and painful to the touch. He couldn’t run around and play but for a few minutes before the pain started, and they he’d have to rest a few days before he could run around with his friends. This was not the life that Brian’s mother wanted for her son. This is not the level of pain a child should have to experience.
Brain was currently under treatment from his rheumatologist, a high dose of methotrexate and naproxen. He would have his liver function tests (LFT) run monthly due to the hepatotoxicity of methotrexate. Brian was used to the blood draws by now, and didn’t fight the phlebotomist like first few times. Brian’s mother came to me desperate. What else could she do for her child? Was this a lifetime of harsh medications that would damage his organs permanently? How could he escape this grim sentence that the rheumatologist said would occur?
JRA affects 70,000 – 100,000 children in the United States. Girls, more commonly than boys, are affected with a 2:1 ratio. Technically, it is defined as a synovial inflammation of at least one joint for at least 6 months. A small percentage of children have ocular complications of cataracts, glaucoma, or loss of vision. Any children with swollen joints should be screened for Lyme and other tick borne infections, regardless of where they live in the country.
Three forms of JRA exist: Pauciarticular, Polyarticular, and Systemic Onset JRA. Pauciarticular makes up 50% of cases and affects fewer than five joints, usually larger joints. Girls normally show a positive ANA, while boys have a positive HLA-B27. Polyarticular, making up 40% of cases, affects more than five joints, and can include weight-bearing joints, such as the neck and hips. It is usually bilateral, and RF+ cases have a worse prognosis. Systemic Onset JRA, making up the remaining 10% of cases, is characterized by high-spiking fevers lasting weeks to months, with a macular rash, affecting smaller joints. This is probably viral in nature.
My first labwork included total IgA levels, which were borderline low 42 (24-121). As with many autoimmune conditions, including JRA, a maladapted gastrointestinal system disrupts the immune system creating a deficiency of mucosal immunity. I often test children and find low IgA levels. This of course predisposes them to intestinal infections, such as C. Diff and candida. While those must be treated if present, they are secondary to the core of the issue and will not provide a permanent resolution. Brian’s candida tests returned negative. The low IgA levels are also usually associated with high IgE levels. Watch these children for allergies, asthma, and eczema. A permanent cure may be obtained by changing the immune system. (Easier said than done…) Brian’s labwork continued. His inflammatory markers were being suppressed by the methotrexate and naproxen. His ESR was 1 and CRP was negative.
To ‘Identify and Treat The Cause’ is a wonderful tenant to strive for, and often one of the most difficult. The more we learn about the physiology of the body, the more we chase and try to tweek with our supplementations and therapy. Are we pulling threads and unraveling the sweater? Let’s take a step back to my favorite drawing, Lindlahr’s Tree of Disease. The trunk of the tree is comprised of:
- Composition of Blood and Lymph
- Accumulation of Morbid Matters
- Strength of the Viz
With the advancements in technology, we can now analyze these more than we could ten or twenty years ago. Philosophically, are we being more or less naturopathic by using the science at hand to identify the cause of disease? Should we use the technology available for the best diagnosis of our patient? It is my opinion that science provides information, and our interpretation of the information is from our paradigm of interpretation. Is the eclipse of the moon from the gods or the physical blocking of light rays…. Or both?
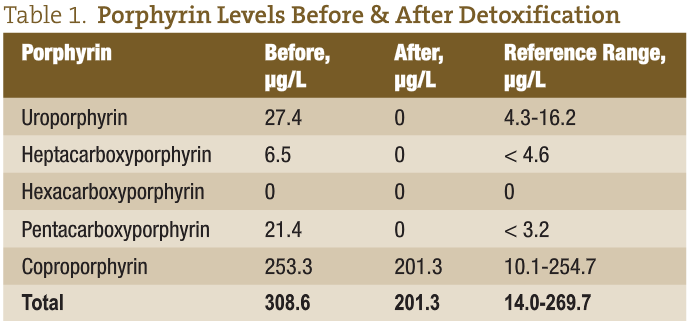
I ordered porphyrin testing to screen for toxicity, as I see this as the cause of many autoimmune as well as neurological conditions in pediatrics. He had elevations of most of them.
Detoxification was obviously going to be part of our treatment, and hopefully would cause a permanent change in the antibody attack of his JRA. I also needed to treat the decrease of immunity in his mucosa, and the assumed inflammation in his intestines. I also needed to protect from liver damage of the methotrexate, as well as treat the folic acid deficiency caused by methotrexate (this medication acts by stopping the methylation of folate).
Treatment began with probiotics and glutamine for the GI, NAC 600mg BID to reverse hepatotoxicity, topical castor oil, quercitin, and oral fish oil to decrease inflammation, homeopathic detoxification liquid, and 5-MTHF 1mg to boost methylated folic acid levels. If you order serum folic acid it will generally be normal in patients taking methotrexate, because the problem is with the methylation, not the absorption.
The months went by and Brian became symptomatically better. While the medications were keeping the inflammation at bay and preventing further destruction of the joints, they were causing problems elsewhere. Our goal was simple and the rheumatologist agreed: stop the medications, if they are not needed. Every office visit we watched for the same things, redness and heat. Every night, Brian’s mother would feel his knees. Were they red? Were they warm?
A few months into treatment, the rheumatologist was ready to take Brian off of medications. First, the naproxen was stopped. No worsening of symptoms. Then the methotrexate was stopped. No worsening of symptoms. We continued our therapy and the amazing happened, Brian was better. The rheumatologist called it “remission”.
It was time to stop the natural therapies. The NAC and 5-MTHF were stopped after the methotrexate was weaned. Probiotics and glutamine were stopped. Detoxification was stopped as his porphyrin labs returned normalized. These are the before and after porphyrin tests over 7 months.
All that remained were castor oil, quercitin, and fish oil. A few more months rolled by. Brian was taking karate lessons and growing by the day. Brian’s mother would flinch every time he got kicked in the knee, but it never got swollen. Checking everyday for warmth and redness, Brian was able to stop the quercitin, fish oil, and castor oil over the next few weeks. Brian’s mom was amazed. The impossible had occurred, transforming from methotrexate and a grim prognosis, to a child with a green belt and still singing Britney Spears ‘hit songs’. Naturopathic medicine saved the day once again, and for a child who was four years old, he had the rest of his life to celebrate.

Dr Jared M Skowron ND
Dr. Jared M. Skowron, ND is full-time faculty at University of Bridgeport where he teaches pediatrics and is founder of the Pediatric & Autism Teaching Clinic. Author of Fundamentals of Naturopathic Pediatrics (CCNM Press) and 100 Natural Remedies For Your Child (Rodale, June 2011), he is vice-president and co-founder of the Pediatric Association of Naturopathic Pediatrics. A graduate of NCNM, his practice is dedicated to the natural treatment of the little ones.

















