
Applying Polyvagal Theory to Treat a Traumatized Patient
JENNIFER BRUSEWITZ, ND
ELIZABETH HOLLOWAY, ND
The polyvagal theory, introduced by Stephen Porges, PhD, in 1995, explains how human adaptive responses are modulated through the autonomic nervous system (ANS). This theory challenges the conventional theory, which describes the ANS as a functionally antagonistic system with sympathetic (“fight or flight”) and parasympathetic (“rest and digest”) modes, by proposing a third functional branch.1 The parasympathetic nervous system, predominantly mediated by the vagus nerve, subdivides in the brainstem into ventral and dorsal vagal tracks. The polyvagal theory postulates that the ventral track induces the “social engagement system,” as illustrated through our ability to connect interpersonally during times of safety; on the other hand, the dorsal track triggers a death-feigning response observed as dissociating or “freezing” during life-threatening situations.2 With this distinction, the polyvagal theory explains how the sympathetic and parasympathetic systems can elicit a trio of adaptive and hierarchal responses – during times of safety, danger, and extreme threat.3
When experiencing a traumatic event, the dorsal vagal track may become activated, resulting in both the immobilization of an individual’s physical body processes and their emotional resiliency.2 In this state, the ability to adapt and ultimately restore physiological and emotional homeostasis is inhibited. To remobilize, the individual must receive safety cues to disengage the dorsal vagal state and revive ventral vagal tone.3 In this case study, we examine a patient who exhibited what may be considered a state of dorsal vagal activation due to a traumatic experience. We sought to provide our patient with the necessary safety cues to defuse her prolonged state of dorsal vagal activation and guide her back to a baseline of social engagement and optimal health.
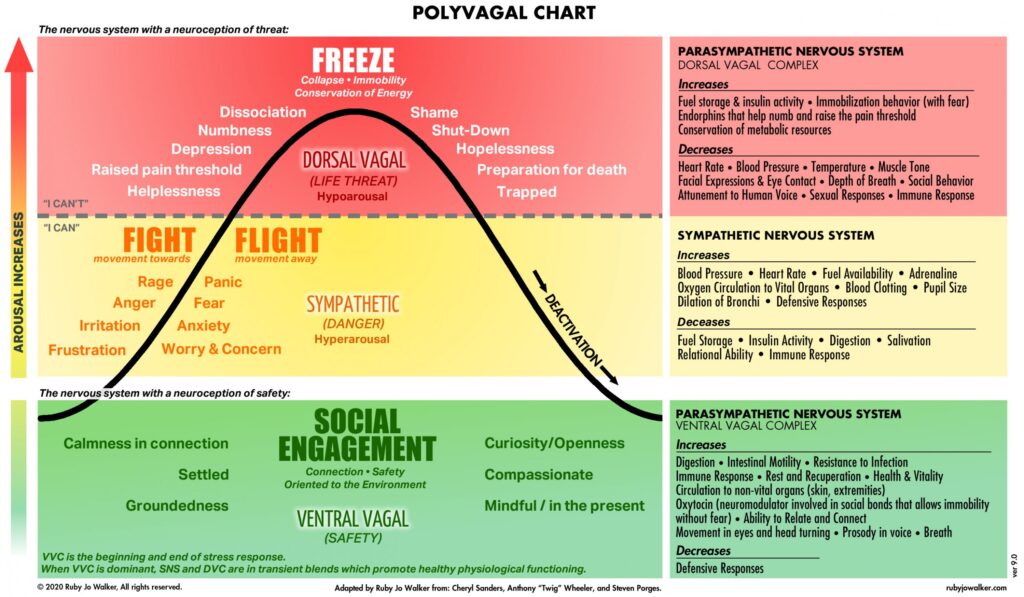
Image courtesy of RJ Walker4
Presenting Concerns & History
A 65-year-old female presented to our clinic with a 17-month history of severe daily migraines, frequently leading to vertigo and vomiting. The patient stated that her headaches inhibited activities of daily living, resulting in a feeling of profound isolation and hopelessness, and prompting an unyielding preoccupation with death. In addition to daily migraines, she reported refractory insomnia, ongoing depression and anxiety, and an intense craving for acidic food. The patient had experienced significant trauma – sexual assault followed by intrusive police interrogation – immediately prior to the onset of her chronic headaches. She was taking sumatriptan daily for migraines, zolpidem as needed for insomnia, and sertraline daily for depression, all of which were prescribed by her primary care physician (PCP).
Clinical Findings
The patient presented with a flat affect, delayed speech, and excessive yawning. She displayed significant difficulty walking and standing upright. Her behavior was cooperative, though communication was slow, revealing cognitive delay. The neurological physical exam elicited no positive findings, and neurological and spinal imaging revealed no abnormalities. Her BMI was 19 and screening blood work was normal except for her HbA1c, which was 5.8%, indicating prediabetes. The questionnaires General Anxiety Disorder-7 (GAD-7) and Patient Health Questionnaire-9 (PHQ-9) revealed moderate anxiety and severe depression.
Therapeutic Interventions
Our treatment goals included migraine relief, sleep improvement, mental health support, and blood sugar regulation. We hoped to reduce the patient’s reliance on sumatriptan for migraines (for which she found minimal symptom reduction) and zolpidem for insomnia (as it left her incapacitated with brain fog, dizziness, and fatigue). In addition, the patient’s use of sertraline was leading to undesirable side effects, such as dizziness and intention tremor, and was not effectively managing her symptoms of depression. Finally, we wanted to reverse her prediabetes status to prevent comorbidities.
Migraine Relief
Craniosacral therapy (CST) is a gentle, hands-on treatment that examines the subtle movement of cerebrospinal fluid and provides a link between the ANS and physical ailments.5 During CST, the practitioner locates and releases areas of physical tension, thereby defusing heightened sympathetic or dorsal vagal responses.5 In this way, CST can rebalance a dysregulated nervous system. Through this approach, we introduced the necessary safety cues to bring about a more regulated nervous system response, supporting the foundation upon which subsequent healing could occur.
Research has shown a correlation between experiencing trauma and increased frequency of migraines, due to trauma’s ability to dysregulate the nervous system.6 Previously believed to be vascular in origin, migraine headaches are now understood as a disorder pertaining to nervous system function; studies indicate reduced sympathetic function among migraineurs and increased susceptibility to migraines among people with abnormal nervous system responses.7 In regulating the nervous system through CST, we sought to decrease the frequency of this patient’s migraines.
In addition, magnesium deficiencies have been linked to migraine development and are believed to be involved in several aspects of migraine pathophysiology. Magnesium induces a calming effect in the body through stimulating gamma-aminobutyric acid (GABA) receptors and limiting glutamate, an excitatory neurotransmitter in the CNS.8 Individuals deficient in magnesium are prone to nervous hyperexcitability, often resulting in migraines.8 Migraineurs with a magnesium deficiency can be treated prophylactically to prevent attacks and reduce debility.8 We prescribed a magnesium supplement in the well-tolerated form of magnesium glycinate to relieve her headaches and their accompanying symptoms.
Sleep Improvement
Next, we sought to improve the patient’s sleep, with the goal of eliminating her need for the use of zolpidem, partly due to its accompanying side effects, which included brain fog, dizziness, and fatigue. Studies show sleep deprivation increases overall morbidity and leads to comorbidities such as depression and diabetes,9 so addressing sleep was a crucial underlying factor to this patient’s overall health. We selected L-theanine as an alternative to promote sleep. L-theanine, an amino acid found in green tea, is thought to reduce the activity of the excitatory neurotransmitter glutamate, allowing for sleep initiation and maintenance.10 Additionally, L-theanine may modulate the levels of monoamines, including serotonin, dopamine, and adrenaline. These compounds typically decrease during sleep in a regulated CNS, resulting in improved sleep quality and quicker recovery from exhaustion, thus allowing the patient to wake feeling refreshed.11
Mental Health Support
The etiology of depression, as with sleep disorders, is often based in a neurotransmitter imbalance.12 Antidepressants attempt to enhance monoamine levels, but their use can lead to adverse effects.13 The patient noted significant side effects coinciding with the initiation of sertraline, including intention tremor, fatigue, dizziness, and insomnia, without a noticeable alleviation of depressive symptoms. We prescribed a supplement that included several monoamine precursors and cofactors, including L-tyrosine and 5-HTP, providing building blocks for endogenous neurotransmitters.12
Blood Sugar Regulation
Lastly, we sought to address the patient’s prediabetes and fatigue, potentially attributed to impaired insulin response. The polyvagal theory explains that in times of threat, dorsal vagal activation triggers increased insulin activity14; it is an advantageous response in the short-term, though if prolonged, can lead to insulin resistance through reduced insulin sensitivity.15 The patient’s diet consisted of meats, rice, vegetables, and fruit. The patient’s labs revealed blood glucose in the prediabetic range, reflecting an insulin resistance picture. To address this, we asked the patient to substitute brown rice for white rice,15 started her on the Ayurvedic herb gymnema (Gymnema sylvestre),16 and prescribed a daily movement regimen.17 Additionally, we suggested the homeopathic remedy Veratrum album, indicated for headache, dizziness, vomiting, and acidic craving,18 as the patient reported juicing 10 tangerines per day. Complex carbohydrates, like brown rice, offer more fiber and a lower glycemic load than white rice or juiced fruit, which spike insulin.15 Gymnema was selected due to its efficacy in regulating blood glucose; when administered to individuals with insulin resistance, gymnema reduced fasting glucose and HbA1c scores and enhanced endogenous insulin.16
Follow-ups & Outcomes
The patient received her first CST treatment, after which she noted the complete resolution of her migraine in the office. She also experienced 10 minutes of incessant yawning following the treatment, and perhaps most importantly, a profound realization regarding the connection between the significant trauma she had experienced and the onset of her chronic headaches, insomnia, and decline in mental health.
At the patient’s week-2 follow-up, she reported following our recommendations without any adverse effects and experienced a noticeable reduction in the duration of her daily migraines. Her cravings for acidic foods had completely resolved, which she described as a huge relief. Symptoms of vertigo also resolved, and headaches had become more intermittent. She was sleeping through the night and her fatigue was improving. The patient also disclosed that her tremor resolved after her PCP discontinued her prescription of sertraline.
At 4 weeks, the patient reported complete resolution of her migraines for an entire day following her second CST treatment, expressing that the absence of the headache allowed her mental health to rebound. In contrast to her previous preoccupation with death, she noticed her thoughts of dying dissolving as her vitality returned. The patient resumed daily activities, including playing piano and yardwork, though she initially noted exhaustion following the exertion. With her hopelessness dissolving, she expressed a desire for ongoing support and connection. She requested CST at each subsequent office visit, conveying her sense of empowerment upon recognizing the connection between her headaches and her nervous system. At additional follow-up appointments, the patient reported greater clarity in cognition, faster processing, and more alertness. She reported increased energy and a renewed ability to multitask. She noted her need to avoid stressful thoughts and emotions as they triggered migraines.
By her 2-month visit, she had begun receiving additional, weekly CST treatments and reported alleviation of migraines for a few days following each session. At this time, she reported increased stress due to ongoing legal proceedings related to the trauma she had experienced, and this resulted in ruminating thoughts leading to insomnia. We addressed sleep hygiene, instructing avoidance of screen time 1 hour prior to bed19; reiterated the importance of daily exercise20; and prescribed melatonin, a hormone thought to regulate the sleep-wake cycle.9 To complement her bedtime routine, we prescribed four-square breathing, another technique that deactivates a heightened sympathetic nervous system response.21
At 4 months, she reported migraines had reduced in severity and finally felt manageable. She noted the use of four-square breathing had completely resolved her insomnia. She expressed renewed cognitive function clarity and stated that her body felt more connected following each CST session. Her PHQ-9 in office revealed her depression had dropped from severe to mild.
Discussion
Traumatic events have the potential to stunt or even immobilize the body through their effects on the nervous system.2 The polyvagal theory illuminates the complex and dynamic mechanisms of human adaptive responses of the ANS. These include the parasympathetic ventral vagal track’s “rest and digest” state that embodies supportive social engagement and cues of safety, the sympathetic nervous system’s “fight or flight” state in response to danger, and the parasympathetic dorsal vagal track’s “freeze” state in response to extreme threat.3 This hierarchy of adaptive responses, necessary for survival in the short-term, can become maladaptive if the system engages a sympathetic or dorsal vagal response that it cannot effectively disengage. Cueing the body’s nervous system with signs of safety becomes essential in defusing an activated state. Subtle body work, such as CST, is an option that can provide the body with signals to downregulate from an excessive state of either sympathetic or dorsal vagal tone. By approaching this patient’s symptoms as a trauma response that led to a dysregulated nervous system, we were able to target our treatment on the underlying cause; with proper safety cues in place, this patient could improve each of her ailments with additional naturopathic support in the form of herbs, nutrients, and lifestyle counseling. We witnessed our patient transform from believing herself at death’s door to ultimately reengaging with life.
[REFS]
- Gibbons CH. Basics of autonomic nervous system function. Handb Clin Neurol. 2019;160:407-418.
- Leikola A, Mäkelä J, Punkanen M. Polyvagaalinen teoria ja emotionaalinen trauma [Polyvagal theory and emotional trauma]. Duodecim. 2016;132(1):55-61.
- Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol. 2001;42(2):123-146.
- Walker RJ. Polyvagal Theory Graphic. Ruby Jo Walker, LCSW; 2021. https://www.rubyjowalker.com/polyvagal_theory.html. Accessed December 10, 2021.
- Girsberger W, Bänziger U, Lingg G, et al. Heart rate variability and the influence of craniosacral therapy on autonomous nervous system regulation in persons with subjective discomforts: a pilot study. J Integr Med. 2014;12(3):156-161.
- Arcaya MC, Lowe SR, Asad AL, et al. Association of posttraumatic stress disorder symptoms with migraine and headache after a natural disaster. Health Psychol. 2017;36(5):411-418.
- Goadsby PJ, Holland PR. An Update: Pathophysiology of Migraine. Neurol Clin. 2019;37(4):651-671.
- Teigen L, Boes CJ. An evidence-based review of oral magnesium supplementation in the preventive treatment of migraine. Cephalalgia. 2015;35(10):912-922.
- Hanson JA, Huecker MR. Sleep Deprivation. In: StatPearls. Treasure Island (FL): StatPearls Publishing; March 7, 2022.
- Rao TP, Ozeki M, Juneja LR. In Search of a Safe Natural Sleep Aid. J Am Coll Nutr. 2015;34(5):436-447.
- Hidese S, Ogawa S, Ota M, et al. Effects of L-Theanine Administration on Stress-Related Symptoms and Cognitive Functions in Healthy Adults: A Randomized Controlled Trial. Nutrients. 2019;11(10):2362.
- Nutt DJ. Relationship of neurotransmitters to the symptoms of major depressive disorder. J Clin Psychiatry. 2008;69 Suppl E1:4-7.
- Ferguson JM. SSRI Antidepressant Medications: Adverse Effects and Tolerability. Prim Care Companion J Clin Psychiatry. 2001;3(1):22-27.
- Filippi BM, Yang CS, Tang C, Lam TK. Insulin activates Erk1/2 signaling in the dorsal vagal complex to inhibit glucose production. Cell Metab. 2012;16(4):500-510.
- Bessesen DH. The role of carbohydrates in insulin resistance. J Nutr. 2001;131(10):2782S-2786S.
- Shanmugasundaram ER, Rajeswari G, Baskaran K, et al. Use of Gymnema sylvestre leaf extract in the control of blood glucose in insulin-dependent diabetes mellitus. J Ethnopharmacol. 1990;30(3):281-294.
- Bird SR, Hawley JA. Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport Exerc Med. 2017;2(1):e000143.
- Morrison R. Desktop Guide to Keynotes and Confirmatory Symptoms. Albany, CA: Hahnemann Clinic Pub.; 1992.
- Li XS, Buxton OM, Lee S, et al. 0803 Insomnia symptoms and sleep duration mediate the association between adolescent screen time and depressive symptoms. Sleep. 2018;41(suppl_1).
- Baron KG, Reid KJ, Zee PC. Exercise to improve sleep in insomnia: exploration of the bidirectional effects. J Clin Sleep Med. 2013;9(8):819-824.
- Ma X, Yue ZQ, Gong ZQ, et al. The Effect of Diaphragmatic Breathing on Attention, Negative Affect and Stress in Healthy Adults. Front Psychol. 2017;8:874.

Jennifer Brusewitz, ND, graduated from the National University of Natural Medicine. She currently practices in Portland, OR, serves as a clinical supervisor at NUNM’s teaching clinics and as academic faculty at NUNM. She also investigates and implements quality assurance standards for the university’s dispensary.

Elizabeth Holloway, ND, is a recent graduate of the National University of Natural Medicine. Prior to attending NUNM, she interned with the US Department of State, taught elementary school in South Korea, and guided horticulture therapy in Hawaii. Elizabeth is passionate about mental health and employing mind-body interventions to regulate the nervous system.

















