Dr. Juline Savaya, ND
Beyond “Unexplained” Recurrent Pregnancy Loss: An Integrative Approach to Immune, Hormonal, Thrombophilic, and Male-Factor Assessment
Pregnancy loss occurs in approximately 15% to 20% of recognized pregnancies, though the true prevalence is likely higher due to underreporting of biochemical pregnancies.1,2 An estimated 23 million miscarriages occur worldwide each year, translating to approximately 44 pregnancy losses every minute.3 A comprehensive recurrent pregnancy loss assessment is critical, as recurrent pregnancy loss (RPL)—commonly defined as two or more pregnancy losses—affects approximately 1% to 2% of couples and carries significant emotional, psychological, and physical consequences.3
Despite its prevalence, many patients with early or biochemical pregnancy losses do not qualify for comprehensive evaluation under conventional standards of care. Patients are often told to “keep trying” or wait until additional losses occur before further investigation is initiated. This creates a significant gap in care, particularly for patients with modifiable endocrine, metabolic, inflammatory, immune, or thrombophilic contributors that may already be present.
Recurrent pregnancy loss is rarely caused by a single factor alone. In clinical practice, endocrine dysfunction, immune dysregulation, insulin resistance, thrombophilic conditions, nutrient deficiencies, endometrial pathology, and male-factor contributors frequently coexist and interact simultaneously. This multifactorial nature highlights the importance of a comprehensive and collaborative approach to assessment and treatment.
Naturopathic doctors are uniquely positioned to help bridge this gap through individualized preconception evaluation, interdisciplinary collaboration, and identification of modifiable risk factors that may impact implantation, placental development, and pregnancy maintenance.
The Multifactorial Nature of RPL
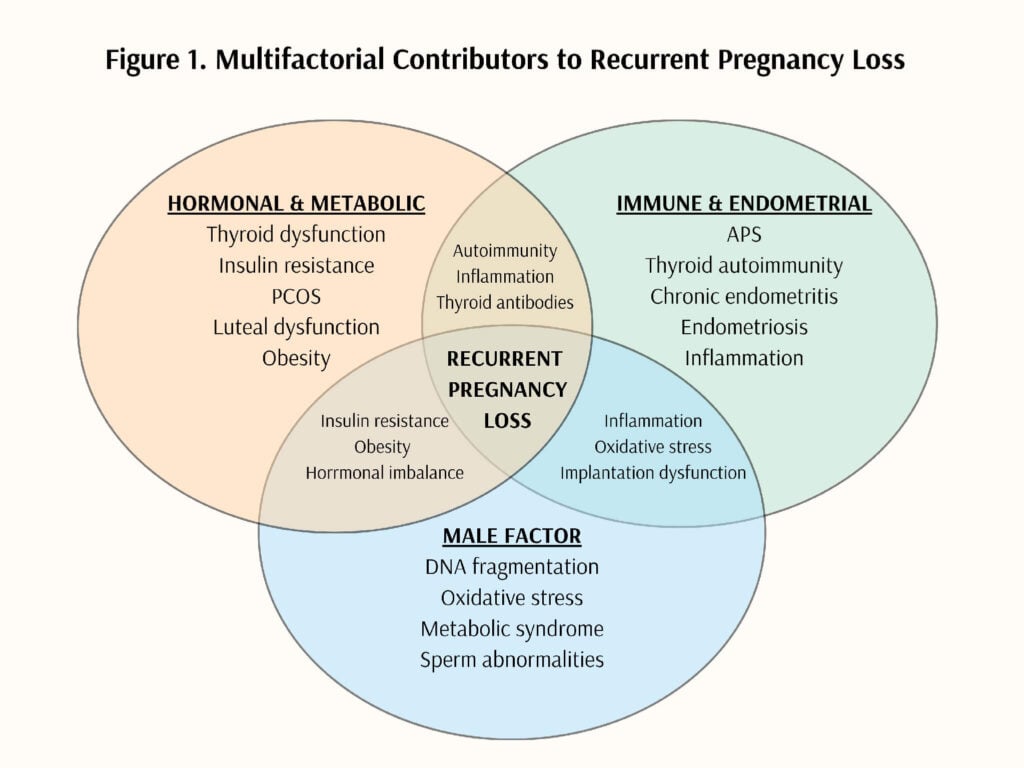
Recurrent pregnancy loss should be viewed as a systemic condition rather than solely a reproductive disorder. Numerous contributors may impair implantation, development of the endometrial lining (decidualization), healthy placental development, embryo development, or immune tolerance during early pregnancy. These contributors may include endocrine dysfunction, autoimmune disease, thrombophilic conditions, metabolic dysfunction, nutrient deficiencies, endometrial pathology, genetic abnormalities, environmental exposures, and male-factor infertility.
Importantly, these factors often overlap. For example, insulin resistance may contribute to chronic inflammation and oxidative stress, while thyroid autoimmunity may coexist with antiphospholipid syndrome (APS), PCOS, or other autoimmune conditions. As a result, identifying and addressing only one contributor may fail to fully reduce future pregnancy risk.
An integrative approach to RPL should therefore focus not only on identifying pathology, but also on optimizing the physiologic environment required for implantation and healthy placental development.
Hormonal & Metabolic Contributors
Hormonal and metabolic dysfunction are increasingly recognized as important contributors to recurrent pregnancy loss, particularly in patients whose prior evaluation has been considered “unexplained.” Thyroid dysfunction, insulin resistance, obesity, polycystic ovary syndrome (PCOS), hyperprolactinemia, and luteal phase abnormalities may impair ovulation, implantation, decidualization, placental development, and immune tolerance within early pregnancy.
In addition to their reproductive effects, endocrine and metabolic dysfunction may contribute to oxidative stress, chronic inflammation, altered endometrial receptivity, and hypercoagulability. Assessment of hormonal and metabolic health may therefore provide important diagnostic and therapeutic opportunities in patients with RPL.
Thyroid Dysfunction & Thyroid Autoimmunity
Thyroid autoimmunity is associated with an increased risk of pregnancy loss, even in patients with otherwise normal thyroid hormone levels.4 Women with recurrent pregnancy loss demonstrate a higher prevalence of thyroid peroxidase antibodies (TPO-Ab) compared to the general reproductive population.4
Thyroid hormones play an important role in oocyte maturation, implantation, placental development, and endometrial receptivity. Inadequate thyroid adaptation during early pregnancy may impair these processes and contribute to pregnancy complications.
Recommended screening may include:
- TSH
- Free T4
- Free T3
- Anti-TPO antibodies
- Anti-thyroglobulin antibodies
Preconception optimization of thyroid function is essential, particularly in patients with thyroid autoimmunity or subclinical hypothyroidism. The American Thyroid Association (ATA) and Endocrine Society recommend maintaining a preconception TSH between 0.5-2.5 mIU/L. Close monitoring during the first trimester is also important, as thyroid hormone requirements commonly increase during early pregnancy.5
Progesterone & Luteal Function
Progesterone plays a central role in implantation, decidualization, immune tolerance, and maintenance of early pregnancy. Several endocrinopathies associated with RPL, including PCOS, prolactin disorders, and chronic stress, may impair luteal progesterone production.
Evaluation should include a detailed menstrual and ovulatory history, including cycle length, luteal phase length, premenstrual spotting, and ovulation tracking. Mid-luteal progesterone testing, ideally performed approximately 7 days after ovulation, may provide additional clinical insight. Mid-luteal serum progesterone reflects corpus luteum function and endometrial receptivity. A level less than 10 ng/mL has been associated with luteal phase defect (LPD) and may be associated with early pregnancy loss in some patients, although diagnostic criteria and interpretation remain debated within the literature.6 Repeat testing across 2-3 cycles may improve clinical accuracy.
Although evidence surrounding progesterone supplementation remains mixed, some studies suggest benefit in patients with recurrent miscarriage or threatened miscarriage, particularly when progesterone is initiated early in pregnancy. In clinical practice, individualized progesterone support may be considered in patients with suspected luteal insufficiency or prior early pregnancy losses.
Insulin Resistance & PCOS
PCOS is associated with an increased risk of pregnancy loss, particularly in the presence of obesity, hyperinsulinemia, and hyperandrogenism.7 However, insulin resistance may contribute to pregnancy loss independently of PCOS or obesity.8
Insulin resistance contributes to chronic inflammation, oxidative stress, altered implantation signaling, and hypercoagulability.9 Hyperandrogenism may impair implantation and placental development, potentially increasing the risk of pregnancy loss.10
Recommended screening may include:
- Fasting insulin, fasting glucose, HOMA-IR, HbA1c
- Lipid panel
- FSH, LH, estradiol, total and free testosterone, DHEA-S
- Mid-luteal serum progesterone
- Prolactin
- 17-hydroxyprogesterone
Clinical management should focus on improving metabolic health and insulin sensitivity through anti-inflammatory nutrition, blood sugar stabilization, movement, sleep optimization, stress reduction, and targeted interventions when appropriate.
Immune & Endometrial Considerations in Recurrent Pregnancy Loss Assessment
Successful implantation and maintenance of early pregnancy rely on a healthy endometrial environment and appropriately regulated immune function. Chronic inflammation, infection, oxidative stress, autoimmune disease, and impaired immune tolerance may all contribute to recurrent pregnancy loss.
Several conditions associated with RPL also overlap with immune dysfunction, including thyroid autoimmunity, vitamin D deficiency, insulin resistance, endometriosis, chronic endometritis, and APS. These conditions may contribute to inflammation, impaired immune regulation, and altered endometrial function, potentially affecting implantation and pregnancy maintenance.
Antiphospholipid Syndrome & Autoimmune Conditions
APS is one of the most well-established immune-mediated causes of recurrent pregnancy loss.11 Screening is generally recommended after two pregnancy losses and may include:
- Lupus anticoagulant
- Anticardiolipin antibodies (IgG/IgM)
- Anti-beta-2 glycoprotein I antibodies (IgG/IgM)
Additional autoimmune evaluation may be considered based on clinical history and presentation, including:
- ANA
- Celiac screening
- Thyroid antibodies
Patients with autoimmune conditions may have impaired immune regulation and increased inflammation within the endometrial environment, potentially affecting implantation and pregnancy maintenance.
Endometriosis & Chronic Endometritis
Chronic endometritis and endometriosis are increasingly recognized as important contributors to recurrent pregnancy loss.12 Chronic endometritis may impair implantation, decidualization, immune tolerance, and placental development through persistent inflammation of the endometrial lining.12 Endometriosis may additionally impair fertility and pregnancy maintenance through altered immune signaling, progesterone resistance, oxidative stress, and abnormal uterine contractility.12
Evaluation may include:
- Endometrial biopsy
- Hysteroscopy
- Pelvic imaging
- Vaginal or cervical cultures when indicated
- Microbiome assessment tools such as EMMA and ALICE
Vitamin D & Immune Regulation
Vitamin D deficiency has been associated with recurrent pregnancy loss and may contribute to altered immune regulation, increased autoantibody production, insulin resistance, and chronic inflammation.13
Assessment of serum 25-hydroxy vitamin D should be considered in patients with recurrent pregnancy loss, particularly in the setting of autoimmune disease, metabolic dysfunction, or chronic inflammatory conditions. In clinical practice, many providers aim to maintain vitamin D levels above 75 nmol/L during preconception and pregnancy.
Male Factor: The Missing Piece
Male-factor assessment is frequently overlooked in recurrent pregnancy loss despite the paternal genome contributing 50% of embryonic DNA. Sperm quality plays a critical role in fertilization, embryo development, implantation, and placental formation.14
Abnormal sperm parameters, including impaired motility, morphology, and elevated DNA fragmentation, have been reported more commonly in couples with recurrent pregnancy loss.14,15 Oxidative stress appears to be a major contributor to sperm DNA damage and may be influenced by smoking, alcohol use, obesity, metabolic syndrome, heat exposure, environmental toxins, inflammation, and nutrient deficiencies.16
A comprehensive male-factor evaluation may include:
- CBC, CMP, lipid panel, HbA1c
- Total and free testosterone, DHEA-S, SHBG
- LH/FSH, estradiol, prolactin
- Thyroid panel
- Vitamin D, ferritin, vitamin B12
- Semen analysis and sperm DNA fragmentation testing
- Parental karyotype when indicated
Lifestyle modification, antioxidant support, reduction of environmental toxicant exposure, and optimization of metabolic health may improve sperm quality and reduce oxidative stress burden.
An Integrative Clinical Framework
Recurrent pregnancy loss requires a comprehensive and individualized clinical framework rather than a singular treatment approach. The goal of integrative care is not simply to maintain pregnancy, but to identify and address the physiologic contributors impairing implantation, placental development, immune tolerance, and embryo development.
Clinical management should focus on:
- Identifying modifiable risk factors
- Optimizing metabolic and hormonal health
- Reducing inflammation and oxidative stress
- Supporting endometrial receptivity
- Addressing nutrient deficiencies
- Improving sperm quality
- Coordinating interdisciplinary care when indicated
Importantly, many contributors to recurrent pregnancy loss are also associated with long-term cardiometabolic and autoimmune disease risk. Early intervention may therefore improve not only pregnancy outcomes, but overall long-term health.
Case Study
A 27-year-old female presented with a history of two pregnancy losses occurring at approximately 5 to 6 weeks gestation. Both losses were classified as biochemical pregnancies confirmed by positive hCG testing without ultrasound confirmation. Because the patient did not meet conventional criteria for recurrent pregnancy loss evaluation, additional workup had not previously been initiated.
Comprehensive laboratory evaluation revealed:
- TSH: 2.2 mIU/L
- Elevated thyroglobulin antibodies
- hs-CRP: 1.7 mg/L
- Ferritin: 21 ng/mL
- Vitamin D: 27 ng/mL
- Homocysteine: 8.8 μmol/L
- Mid-luteal progesterone: 7.5 ng/mL
Although ovulation was confirmed, progesterone levels were considered suboptimal for adequate luteal support. Additional findings suggested underlying inflammatory burden, nutrient insufficiency, and thyroid autoimmunity.
Treatment focused on comprehensive preconception optimization and included:
- Mediterranean-style anti-inflammatory nutrition
- Stress management and sleep support
- Omega-3 fatty acids
- Vitamin D and iron supplementation
- Prenatal nutrient support
- Luteal progesterone support beginning after ovulation
The patient was additionally educated on fertility awareness and ovulation tracking to better identify timing of ovulation and luteal phase support.
Approximately 5 weeks after beginning treatment, the patient reported a positive pregnancy test. Follow-up laboratory testing demonstrated appropriately rising hCG levels and improved progesterone levels. The patient continued progesterone support through the first trimester while receiving collaborative prenatal care alongside her OB/GYN.
She ultimately carried the pregnancy to term and delivered a healthy infant.
This case highlights the importance of early evaluation and individualized preconception care in patients with biochemical pregnancy loss who may not otherwise qualify for comprehensive recurrent pregnancy loss assessment under conventional guidelines.
Conclusion
Recurrent pregnancy loss is a complex and multifactorial condition that extends beyond reproduction alone. Endocrine dysfunction, immune dysregulation, metabolic health, thrombophilic conditions, nutrient deficiencies, endometrial pathology, and male-factor contributors may all influence implantation, placental development, and pregnancy maintenance.
Conventional standards of care may fail to identify important contributors in patients with early or biochemical pregnancy losses. Naturopathic doctors are uniquely positioned to help bridge this gap through comprehensive assessment, interdisciplinary collaboration, and individualized preconception optimization.
Early identification of modifiable contributors may not only improve pregnancy outcomes, but also reduce long-term inflammatory, metabolic, cardiovascular, and autoimmune disease risk for both parents.
References
- Alves C, Jenkins SM, Rapp A. Early pregnancy loss (spontaneous abortion). In: StatPearls. StatPearls Publishing; 2023. Accessed May 16, 2026. https://www.ncbi.nlm.nih.gov/books/NBK560521/
- Kratz B, Rasheed A, Holden JP. Luteal phase support for documented failure of placental steroidogenesis: a case report. Case Rep Womens Health. 2016;14:1-3. doi:10.1016/j.crwh.2016.12.002
- Quenby S, Gallos ID, Dhillon-Smith RK, et al. Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet. 2021;397(10285):1658-1667. doi:10.1016/S0140-6736(21)00682-6
- Xie J, Liu Y, Zeng X, et al. Effect of antithyroid antibodies on women with recurrent miscarriage: a meta-analysis. Am J Reprod Immunol. 2020;83(5):e13238. doi:10.1111/aji.13238
- Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017;27(3):315-389. doi:10.1089/thy.2016.0457
- Practice Committee of the American Society for Reproductive Medicine. Diagnosis and treatment of luteal phase deficiency: a committee opinion. Fertil Steril. 2021;115(6):1416-1423. doi:10.1016/j.fertnstert.2021.02.010
- Sun YF, Zhang J, Xu Y, et al. High BMI and insulin resistance are risk factors for spontaneous abortion in patients with polycystic ovary syndrome undergoing assisted reproductive treatment: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2020;11:592495. doi:10.3389/fendo.2020.592495
- Craig LB, Ke RW, Kutteh WH. Increased prevalence of insulin resistance in women with a history of recurrent pregnancy loss. Fertil Steril. 2002;78(3):487-490. doi:10.1016/S0015-0282(02)03247-8
- Wang Y, Zhao H, Zhang H, et al. Relationship between recurrent miscarriage and insulin resistance. Gynecol Obstet Invest. 2011;72(4):245-251. doi:10.1159/000324794
- Wang K, et al. Hyperandrogenism increases late spontaneous miscarriage in polycystic ovary syndrome women due to cervical insufficiency? A propensity-score matching study. BMC Pregnancy Childbirth. 2025;25:172. doi:10.1186/s12884-025-07342-4
- Abrahams VM, Chamley LW, Salmon JE. Antiphospholipid syndrome and pregnancy: pathogenesis to translation. Arthritis Rheumatol. 2017;69(9):1710-1721. doi:10.1002/art.40136
- Pirtea P, Cicinelli E, De Nola R, et al. Endometrial causes of recurrent pregnancy losses: endometriosis, adenomyosis, and chronic endometritis. Fertil Steril. 2021;115(3):546-560. doi:10.1016/j.fertnstert.2020.12.010
- Ota K, Dambaeva S, Han AR, et al. Vitamin D deficiency may be a risk factor for recurrent pregnancy losses by increasing cellular immunity and autoimmunity. Hum Reprod. 2014;29(2):208-219. doi:10.1093/humrep/det424
- Gil-Villa AM, Cardona-Maya W, Agarwal A, Sharma R, Cadavid A. Assessment of sperm factors possibly involved in early recurrent pregnancy loss. Fertil Steril. 2010;94(4):1465-1472.
- Dai Y, Wang Y, Li X, et al. Relationship among traditional semen parameters, sperm DNA fragmentation, and unexplained recurrent miscarriage: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2021;12:802632.
- Majzoub A, Agarwal A. Systematic review of antioxidant types and doses in male infertility. Arab J Urol. 2018;16(1):113-124.
 About the Author: Dr. Juline Savaya, NMD, is a licensed naturopathic physician in Arizona specializing in fertility, women’s health, thyroid disorders, and metabolic dysfunction. She earned her doctorate in naturopathic medicine from Sonoran University of Health Sciences and completed postgraduate training in women’s health. Dr. Savaya is founder of Juline Savaya Naturopathic Wellness and Jade Holistic Health Center. Follow her on Instagram & TikTok: @drjulinesavaya
About the Author: Dr. Juline Savaya, NMD, is a licensed naturopathic physician in Arizona specializing in fertility, women’s health, thyroid disorders, and metabolic dysfunction. She earned her doctorate in naturopathic medicine from Sonoran University of Health Sciences and completed postgraduate training in women’s health. Dr. Savaya is founder of Juline Savaya Naturopathic Wellness and Jade Holistic Health Center. Follow her on Instagram & TikTok: @drjulinesavaya