Regenerative Medicine
Fred G. Arnold, DC, NMD
Palpation-guided injections have been the method for administering regenerative joint injections for decades. Ultrasound-guided injections have been gaining in popularity as technology and practitioners’ skills have improved. Each of these injection methods has both advantages and disadvantages.
Currently, there are a variety of different regenerative joint solutions that are being used in practice: prolotherapy, prolozone, platelet-rich plasma (PRP), adipose stem cells, bone marrow concentrate stem cells (BMAC), amniotic tissues, alpha-2-macroglobulin, and exosomes. These different regenerative joint solutions may be used alone or in combination to improve efficiency.
Palpation- or Landmark-Guided Injections
Palpation is an art that involves manual examination of a body to determine its size, shape, firmness or location. Musculoskeletal palpation is used to identify the location and abnormalities of different joints in order to perform palpation-guided injections; it has been the standard for regenerative joint injections for decades. Regenerative joint practitioners are trained to successfully perform palpation-guided regenerative joint injections such as prolotherapy, PRP, prolozone, and stem cells. In addition to relying on palpation skills, practitioners utilize patient history and diagnostic tests such as X-ray and MRI. Most of the areas to be injected are painful on palpation, which is helpful to the practitioner in determining where to inject. Palpation-guided injections require a strong understanding of human anatomy.
Advantages of Palpation/Landmark-Guided Injections:
- Neither patient nor doctor bears the cost burden of an ultrasound machine.
- Palpations-guided injections have been successfully performed for decades.
- This kind of injection is easier to learn than ultrasound-guided injections.
Disadvantages of Palpation/Landmark-Guided Injections:
- Exact needle placement may not always be achieved.
- Patient outcome can be compromised by an inexperienced practitioner.
- Diagnosis of underlying structures is not always accurate.
Ultrasound-Guided Injections
Using the ultrasound for musculoskeletal conditions has become increasingly popular over the past few years for both diagnosis and guided injections. Orthopedic Training organizations – such as the American Association of Orthopedic Medicine, The Hackett-Hemwell Foundation, and the American Osteopathic Association of Prolotherapy Regenerative Medicine – now teach ultrasound-guided injections as part of their training for regenerative joint injections. Some ultrasound-training institutions now offer specific training for treatment of musculoskeletal conditions, and private companies will send experienced technicians to a doctor’s office to assist them with specific injection procedures.
Advantages of Ultrasound-Guided injections:
- Exact visual identification of the structure to be injected is possible, as well as immediate assessment of the structures to be injected.
Figure 1. Anterior hip joint

Of all the joints in the body, the hip joint can be the most difficult to treat when there is moderate-to-advanced degeneration and arthritis. Ultrasound enables exact placement of the injection needle within the joint capsule.
- Ultrasound allows for identification of anatomical structures for exact needle placement.
Figure 2. Suprapatellar recess above knee cap

The suprapatellar recess above the knee cap is exactly where the needle should be placed for an intra-articular injection of the regenerative joint solution.
- Ultrasound allows for identification of structures that would not benefit from regenerative joint injections.
Figure 3. Image of structure that would not benefit

The picture shows the biceps tendon (arrow) out of the bicipital groove due to a distended and torn transverse humeral ligament.
- Diagnosis can be made of the underlying structures, such as the tendons, ligaments, cartilage, and bone.
Figure 4. Supraspinatus tendon of shoulder

The picture shows the supraspinatus tendon of the shoulder and surrounding tissues.
- Comparison views of anatomical structures are readily available.
Figure 5. Right median nerve (0.11 cm2)
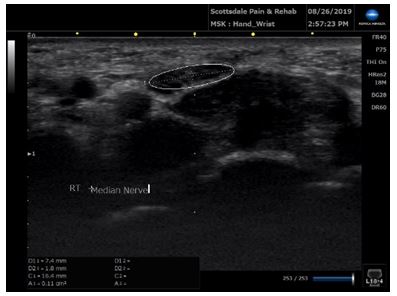
A median nerve area of less than 0.06 cm2 usually excludes carpal tunnel syndrome, whereas an area greater than 0.12 cm2 usually indicates carpal tunnel syndrome.1
Figure 6. Left median nerve (0.09 cm2)
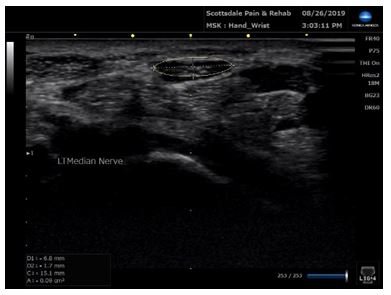
A median nerve area of less than 0.06 cm2 usually excludes carpal tunnel syndrome, whereas an area greater than 0.12 cm2 usually indicates carpal tunnel syndrome.1
- Ultrasound-guided injections are more accurate overall than palpation- or landmark-guided injections. Although studies are limited, ultrasound-guided injections of both upper and lower extremities have been shown to produce greater benefit compared to landmark-guided injections. In one study, upper extremity injections included the glenohumeral joint, the subacromial space, the biceps tendon sheath, and the joints of the hand and wrist. Lower extremity injections included the knee, ankle, and foot.2
- Ultrasound-guided injections are reimbursed by some insurance companies.
- There is no radiation exposure (as opposed to X-ray and computerized tomography).
- Structures such as tendons are moving in real time, thereby revealing functionality of structures and range of motion. Movement of a body part, for example, can help reveal tears, structural displacements, and anatomical anomalies.
- Patients appreciate it when the practitioner can show them the nature of their problem area as well as compare their progress over time using regenerative joint injection therapies.
Disadvantages of Ultrasound-Guided Injections:
- There is a steep “learning curve” in becoming able to identify the structures to be injected. One way to reduce the learning curve is for the practitioner to hire a trained registered musculoskeletal sonographer (RMSKS) on a regular basis. Although ultrasound training is provided at Regenerative Medicine conferences, the amount of actual “hands-on” training is limited, and the workshops are often overcrowded.
- For the practitioner there is the additional cost of the ultrasound machine, which can range from approximately $30K to $50K or more. This can be offset if the office files insurance or charges the patient an additional fee to use the ultrasound machine.
- There may be an additional patient cost for the treatment. So far, we have not had any patients complain about this additional cost. They seem to appreciate the improved accuracy and superior results.
- Evaluation of intra-articular structures is limited. These structures cannot be viewed with ultrasound; however, it is possible to form an opinion of a structure based on extra-articular tissues. Example: a torn meniscus in the knee could present with an extrusion at the joint space and fluid. This is called a “geyser sign.”
- The field of view is limited due to the placement of the probe. However, the probe can easily be moved to view adjacent structures.
Studies
Ultrasonography for the evaluation and treatment of musculoskeletal conditions is an emerging tool in the field of orthopedics. As with any new method in medicine, the number of initial studies comparing landmark-guided injections to ultrasound-guided injections is still limited, and they vary in the accuracy and benefits of each type of injection.
In a study involving diagnostic injection of the shoulder, the authors state, “Accuracy is often improved with the use of ultrasonography guidance, although studies differ on the benefits of guided versus unguided injection.”3 In another study, which involved a comprehensive review of the literature, guided injections of the shoulder glenohumeral joint were associated with higher overall accuracy compared to blind injections. However, as the authors stated, “Nevertheless, in some studies, including a relatively large number of shoulders, blind injections have been proven to be 100% accurate.”4 In a study involving 50 hips that were injected with a contrast, the ultrasound-guided intra-articular hip injections were shown to be “accurate, efficient, and patient-friendly.”5
In other studies involving different anatomical structures, both living and cadaveric, the results supported the accuracy and diagnostic benefits of ultrasound-guided injections for the sacroiliac joint,6 shoulder girdle,7 hip,8 and knee.9 Ultrasound-guided injections have even been shown to be more accurate and provide greater diagnostic benefits than unguided or fluoroscopy-guided biceps tendon sheath injections.10
As would be expected, the accuracy of ultrasound-guided injections is dependent on the user’s degree of experience with the methodology.11
One common conclusion from most of the studies is the need for future clinical studies to compare outcomes of palpation/landmark-guided vs ultrasound-guided injections.
Conclusion
Regardless of the research studies, practitioners should have a firm knowledge of anatomy landmarks as they begin to learn musculoskeletal ultrasound. Palpation skills for performing landmark-guided injections will be of benefit when ultrasound-guided injections are utilized.
The practitioner should be able to perform both palpation-guided injections and ultrasound-guided injections. Palpation should always be performed before any type of injection to ensure proper needle placement. Regardless of the method used, regenerative joint injections provide an attractive alternative to other forms of musculoskeletal treatment, such as physical therapy, steroid injections, or surgery. The side effects of steroid injections should be reviewed before such injections are performed, and surgery should be the last resort for any musculoskeletal procedure.
Richard Kates, RMSKS, provided assistance regarding the identification and accuracy of some of the ultrasound pictures presented.
References:
- Jacobson JA. Fundamentals of Musculoskeletal Ultrasound, 3rd Edition. Philadelphia, PA: Elsevier; 2018: 204.
- Daniels EW, Cole D, Jacobs B, Phillips SF. Existing Evidence on Ultrasound-Guided Injections in Sports Medicine. Orthop J Sports Med. 2018;6(2):2325967117756576.
- McFarland E, Bernard J, Dein E, Johnson A. Diagnostic Injections About the Shoulder. J Am Acad Orthop Surg. 2017;25(12):799-807.
- Simoni P, Grumolato M, Malaise O, et al. Are blind injections of gleno-humeral joint (GHT) really less accurate imaging-guided injections? A narrative systematic review considering multiple anatomical approaches. Radiol Med. 2017;122(9):656-675.
- Balog TP, Rhodehouse BB, Turner EK, et al. Accuracy of Ultrasound-Guided Intra-articular Hip Injections Performed in the Orthopedic Clinic. Orthopedics. 2017;40(2):96-100.
- De Luigi AJ, Saini V, Mathur R, et al. Assessing the Accuracy of Ultrasound-Guided Needle Placement in Sacroiliac Joint Injections. Am J Phys Med Rehabil. 2019;98(8):666-670.
- Aly AR, Rajasekaran S, Ashworth N. Ultrasound-guided shoulder girdle injections are more accurate and more effective than landmark-guided injections: a systematic review and meta-analysis. Br J Sports Med. 2015;49(16):1042-1049.
- Lynch TS, Oshlag Bl, Bottiglieri TS, Desai NN. Ultrasound-Guided Hip Injections. J Am Acad Orthop Surg. 2019;27(10):e451-e461.
- Lueders DR, Smith J, Sellon JL. Ultrasound-Guided Knee Procedures. Phys Med Rehabil Clin N Am. 2016;27(3):631-648.
- Petscavage-Thomas J, Gustas C. Comparison of Ultrasound-Guided to Fluoroscopy-Guided Biceps Tendon Sheath Therapeutic Injection. J Ultrasound Med. 2016;35(10):2217-2221.
- To P, McClary KN, Sinclair MK, et al. The Accuracy of Common Hand Injections With and Without Ultrasound: An Anatomical Study. Hand (N Y). 2017;12(6):591-596.
 Fred G. Arnold, DC, NMD, specializes in Regenerative Joint Injections and has over 28 years of clinical experience. Dr Arnold is certified in prolotherapy by the American Association of Orthopedic Medicine (AAOM), and is also certified in chelation therapy. He is also a Fellow in both the Anti-Aging & Regenerative Medicine and the American Academy of Ozonotherapy (FAAOM). Dr Arnold has degrees in both naturopathic medicine and chiropractic.
Fred G. Arnold, DC, NMD, specializes in Regenerative Joint Injections and has over 28 years of clinical experience. Dr Arnold is certified in prolotherapy by the American Association of Orthopedic Medicine (AAOM), and is also certified in chelation therapy. He is also a Fellow in both the Anti-Aging & Regenerative Medicine and the American Academy of Ozonotherapy (FAAOM). Dr Arnold has degrees in both naturopathic medicine and chiropractic.



