
Vis Medicatrix Naturae
Deborah Ardolf, NMD
In the United States, Autologous (or Autogenous) Urine Immunotherapy (AUIT) is a treatment involving the use of one’s own urine as an immune modulator, with an action quite similar to a homeopathic isode. The active immune modulators, ie, mostly immunoglobulins, are filtered out of the urine and given back to the patient in the form of an intramuscular injection. The treatment was reported back in 1918 as a highly effective and safe treatment by Charles Duncan, MD in his book, Autotherapy.1 Dr. Duncan initially treated animals perceived to be untreatable by modern medicine at the time by developing his own filtration system. Despite the cryptic nature of the apparatus, it worked! Much to his surprise, the test animals not only healed from their lesions, but appeared stronger and more vital than prior to the treatment and lived beyond their expected years. Dr. Duncan went on to conduct classes for over 1000 veterinarians and medical doctors on the correct filtration and AUIT methodology of treatment.
Warp speed to 1982, when Dr. William Hitt wrote a chapter on “Immuno-Tolerance” in the Physician’s Handbook.2 Hitt elucidated the historical and extremely limited knowledge of how an “allergy” was defined for much of the 19th century. As more scientific evaluative equipment became available, the definition evolved, however many of the treatment approaches did not follow suit. It was not uncommon for allergists, internists, pediatricians, and otolaryngologists to have little concept of the role immunology plays in creating an allergic disease. It was not part of their curriculum, even though as early as 1958, low molecular-weight proteins, similar to serum proteins, were found in the urine that were subsequently identified as IgG-related proteins—a heterogeneous mixture of kappa and lambda light chains, HLA antigens, and antibody receptors. Furthermore, Dorner and Uhr,3 discovered that fractions of these proteins, extracted from urine and re-vaccinated, had the ability to inactivate, through binding to an antigen receptor, a specific pathogen. Even though all of this knowledge and data lies before us, our approach to treating illness often continues to lean toward aborting acute symptomatology without necessarily aborting the disease process. When this happens, the root cause of an illness remains uncovered and the patient may never be free of his or her symptoms and disease.
As Dr Hitt so clearly wrote,
“The scientific physician has a primary duty to research new and old procedures and drugs and give objective evaluations. The scientific physician is remiss, if he does not keep an open mind and explore new therapeutic modalities or verify the observations of the clinician. Certainly the clinician is obligated to follow up on the scientist’s data and apply them judiciously in his/her practice. This mutual cooperative effort would not only benefit the medical community, but would translate into mankind’s wellbeing which should be, but sadly is not always, the goal of all physicians”.2
Hypothesis
Over the last 60 years, health care in the United States has continued to move away from natural methods toward pharmaceutical agents. The result is an uncontrollable escalation of health care costs and a new set of complex diseases. Examples include autoimmune diseases such as arthritis and lupus; many are considered incurable. As NDs, we often note the underlying causes of such disorders to be allergenic in nature. Dr. Hitt predicted that by the late 1980s everyone would present with an allergy, primarily due to the number of chemicals introduced into our world. Clinically, this appears to be correct. Allergies are on the rise. A 2013 study,4 conducted by the Centers for Disease Control, showed that the prevalence of food allergies in American children increased from 3.4% in 1997, to 5.1% in 2011. Skin allergies rose more sharply, from 7.4% to 12.5% within the same time period. Arizona used to be the state that people suffering from allergies moved to, often by physician recommendation. It is now difficult to find an allergy-free location. In addition, most patients no longer present with only one chief complaint. Rather, the majority present to the office with an array of health problems, some clearly iatrogenically-induced. It is up to the physician to prioritize, sort out relationships between diseases, and map out the best corrective actions.
The only other AUIT study completed on a patient population who suffered from allergies was a seemingly unpublished chart review of 208 charts from 1977 to 1979 by a research assistant named Joseph Chen, a student at the University of Arizona. After exclusions, only 41 charts contained enough information to proceed. The results of his study reported in Dr. Hitt’s chapter on Immuno-tolerance were impressive. His findings noted a 60% to 94% improvement from AUIT in the typical allergic-type symptoms, ie, runny nose, itchy, burning eyes, skin rashes, hives, etc. Furthermore, these improvements were noted in as few as 8 injections!
This study raises the question of whether AUIT treatments are powerful enough to override a patient’s past exposure to the plethora of pharmaceutical agents and environmental toxins in the world today. Can AUIT still provide complete resolution of symptoms without a patient having ongoing dependency on pharmaceutical, nutraceutical, or AUIT treatments? If so, what is the estimated length of these treatments? Clinical observations suggest clear improvements in symptomatology.
Study Design
It is with these questions in mind that a chart review was conducted of all patients who primarily received AUIT treatment at the clinic of Dr. Ardolf and Associates, LLC, from the period of 2009 to 2012. A total of 344 patient charts were reviewed. Data included patients’ age, gender, primary diagnosis, symptoms at the time of the initial consultation, the number of AUIT treatments, and the symptoms at the time this review ended (January, 2013). Seven patients who chose not to continue the treatment were excluded from the study.
As part of their naturopathic medical care, the patients also received dietary recommendations and supplementation for symptom relief. Some patients in the “complex disease” group received additional naturopathic treatments, depending on their initial chief complaints.
In an attempt to simplify the study, the subjects were then classified according to their primary diagnosis and placed into 1 of the following 5 categories; Allergies, Gastrointestinal, Complex diseases, Migraines, and Acne. As noted earlier, assigning an individual to a specific group was difficult, as many patients presented with multiple disease processes. For example, patients with gastrointestinal issues or acne may have also presented with allergies. The most complex group consisted of patients who presented to the clinic with one or more disorders of the immune system, such as a previously diagnosed autoimmune disease (eg, lupus or multiple sclerosis), fibromyalgia, Lyme disease, cancer, or multiple chemical sensitivities. Often the initial consultation would also uncover other ailments, such as gastrointestinal imbalances, skin rashes, a history of allergies, insomnia, pain, or cachexia,. These complex patients received more treatments than AUIT; however, the AUIT treatments were still a major portion of the treatment plan.
To determine the effectiveness of the treatment, the patients’ symptoms at baseline were compared to their symptoms at the end of treatment. Those still undergoing once-weekly injections at the completion of the data collection were still included in the study, as reflected in Table 1. Data analysis was conducted on those who reported 3 or more symptoms at the time of the initial consultation and resolution of either one or all symptoms by the end of the data collection.
Results
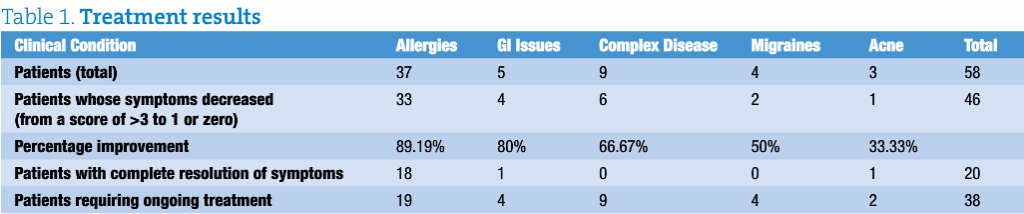
A total of 344 charts were analyzed. Of these, 58 fit the criteria described above. A total of 37 patients had an allergy as their primary diagnosis. With AUIT, 33 patients experienced a decrease in symptoms, from 3 or more, down to 1 or complete resolution of their symptoms. This equated to an 89% improvement in the allergy group! In patients with gastrointestinal issues, an 80% improvement was observed, with only one subject continuing to undergo treatment at the completion of the data collection. Only 50% of the patients with migraines improved; however, further analysis of the data revealed that all subjects in this group were continuing to receive treatment by the completion of the study. The same held true for the acne group; only one participant experienced complete resolution of symptoms, and 2 continued to undergo treatment (Table 1).
In this study, the number of treatments was not limited. Ie, all participants had the option of continuing their treatment until they were satisfied with the reduction in their symptoms and/or were free of disease. Patients in the allergy group required 3 times as many treatments as the allergy patients in Chen’s 1977-1979 study. Patients in the complex disease group required the most treatments to ameliorate their symptoms (Table 2).

The age of the patient influenced the number of treatments required to obtain resolution of symptoms. The younger patients, such as those in the acne group, required fewer treatments than the others. In contrast, the older-age patients, such as those in the complex disease group, required a greater number of treatments (Table 3).

Discussion
As more has been learned about the complexity of allergic responses, which quickly expanded beyond the Type I hypersensitivity response to include the Type V hypersensitivity response (in which antibodies are produced that are directed to specific cell targets), it has become clear that conventional methods of assessment and treatment do not always effectively address a patient’s symptoms or eradicate the disease. Nonetheless, they continue to be used. Because urine contains numerous substances that impact immune function (including both suppressor- and enhancer immunoglobulins, and compounds that are antigen-specific or antigen-independent,5 AUIT appears to be one of the most effective immune modulators available. Repeated injections stimulate the production of memory cells that promote non-reactivity, ie, a symptom-free state otherwise known as “tolerization” in the literature. Treating the underlying cause(s) of disease is the cornerstone of naturopathy.
Early onset of treatment, as noted in both studies, appeared to significantly decrease the length of treatment required to eradicate symptomatology. The older patients had consulted a plethora of physicians and tried many treatment approaches, without improvements in health and well-being. In fact, the opposite often occurred, as patients presented with a host of disease processes. These patients are more difficult to treat. They are slower to respond and often required a smaller increase in the prescribed dosage to reach a symptom-free state. Nonetheless, when you consider treatments such as inhalers, corticosteroids, and other immunosuppressive agents, which often produce side effects and are prescribed for long periods of time, AUIT represents an attractive and inexpensive approach that is likely to ameliorate symptoms and provide a patient with an improved quality of life. The majority of participants in this study experienced symptom improvement from AUIT treatments. None of the patients in the study required hospitalization or needed to abort the treatment due to negative side effects. A longitudinal study is needed to determine if the patients might also benefit from increased life-span.
 Deborah Ardolf, NMD, is a licensed naturopathic physician, who obtained her doctorate from SCNM in 2009. She holds a Masters degree in Speech Pathology, and has completed a fellowship at the Seattle VA Hospital in Geriatrics, an externship with Dr. Hitt, and a preceptorship with Dr. Kruzel. She currently is the founder and owner of Dr. Ardolf and Associates, LLC in Scottsdale, AZ. Her passion is to uncover the root cause of illness using naturopathic principles most of which she has discovered buried deep in the literature.
Deborah Ardolf, NMD, is a licensed naturopathic physician, who obtained her doctorate from SCNM in 2009. She holds a Masters degree in Speech Pathology, and has completed a fellowship at the Seattle VA Hospital in Geriatrics, an externship with Dr. Hitt, and a preceptorship with Dr. Kruzel. She currently is the founder and owner of Dr. Ardolf and Associates, LLC in Scottsdale, AZ. Her passion is to uncover the root cause of illness using naturopathic principles most of which she has discovered buried deep in the literature.
References
- Duncan CH. Autotherapy Self-published; 1918.
- Hitt, W. Immuno-tolerance. In: Krupp MA, Tierney LM, Jawetz E, Roe RL, Camargo CA, eds. Physician’s Handbook. 20th ed. Los Altos, CA: Lange Medical Publications;1982.
- Dorner MM, Uhr JW. Immunologic Tolerance After Specific Immunization” J Exp Med. 1964;120:435-447.
- Jackson KD, Howie LD, Akinbami LJ. Trends in allergic conditions among children: United States, 1997-2011. NCHS Data Brief. 2013;121:1-8.
- Immune Therapy With A.U.I.T. Courtesy of Wm. Hitt, MD, PhD. Arrowhead Healthworks, Lake Arrowhead, CA. http://www.arrowheadhealthworks.com/AUIT.htm. Accessed May 30, 2013.












