Keith Spaulding, ND, MAc, MSEE
The change in the medical worldview due to the invention and widespread use of antibiotics wasn’t just a shift in use from more natural substances to pharmacological substances; it was also a shift away from multiple types of therapeutic tools (electrical, thermal, herbal, food), toward more biochemical solutions. Modern-day naturopathic medicine relies heavily on ingested or injected medicines as therapeutic tools, and relies less on physical therapeutic modalities such as acupuncture, physical medicine, hyperbaric chamber, etc. However, electrical neurostimulation is gaining in the medical world, thanks to a large and growing body of research, and it forms the foundation for an effective and versatile therapeutic. The most researched form of electrical neurostimulation in the last decade is Transcranial Direct Current Stimulation (tDCS).
History of Electrical Neurostimulation
The use of electrical neurostimulation as a therapeutic tool states back to the Roman times; however, its use began to grow in the 1800s with an overall exploration of the use of electromagnetics for the human condition. Luigi Galvani and Alessandro Volta laid the foundation of bioelectricity in the late 1700s by studying the effects of electricity on animals. But it is Giovanni Aldini, in the early 1800s, who is credited for delivering electrotherapy to the brain to treat melancholia. The levels of current used were very high, more akin to electroconvulsive therapy (ECT). Aldini was also regarded as a bit of a charlatan, making himself known by sending large currents through cadavers to “raise the dead”; this probably did more harm for the science than benefit.
In the 1960s, tDCS research resurfaced in the investigation of cortical plasticity in animals; however, the stimulation levels were not consistent, and the research seemed to ebb. Later, in the early years of this century, researchers at the Georg-August University in Goettingen, Germany – particularly Michael Nietsche and Walter Paulus – began to spearhead the new movement in tDCS by finding sustained cortical excitability elevations in humans through the application of direct current therapy to the brain.1 As the electrophysiological effect of tDCS became better known, the research shifted more towards its clinical effects.
There has been a surge in tDCS research within the last 10 years or so (see Figure 1). Of course, these studies are not all clinical research. The research can be broadly separated into investigations of healthy participants (mostly examining cognitive enhancement benefits of tDCS) and investigations of those with a clinical condition (examining the full range of neurological conditions).
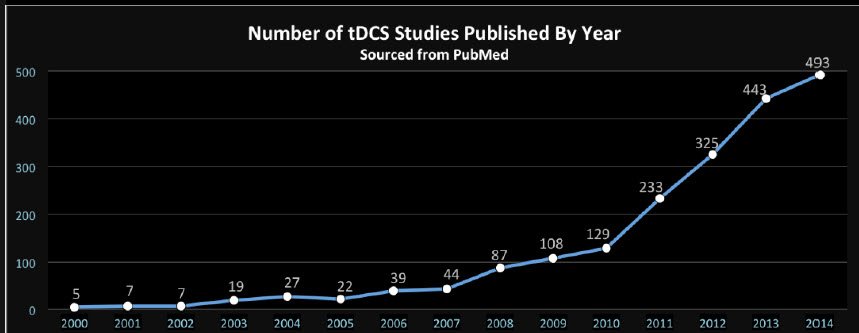
Figure 1. Growth of Research in tDCS Studies
In terms of clinical investigation, the most prevalent research – and the most successful – appears to be in the areas of in depression, stroke, and pain. Table 1 shows PubMed results using a defined search.
Table 1. PubMed Search of tDCS Topics
| Search Terms | # of Results |
| tDCS AND Learning | 322 |
| tDCS AND Stroke | 288 |
| tDCS AND Memory | 214 |
| tDCS AND Depression | 208 |
| tDCS AND Pain | 162 |
| tDCS AND Safety | 108 |
| tDCS AND Cognitive Enhancement | 55 |
| tDCS AND Bipolar | 31 |
| tDCS AND Parkinson’s | 25 |
| tDCS AND Alzheimer’s | 13 |
(PubMed search conducted January, 2015)
Experimentations with tDCS
I am a former naturopathic doctor that has migrated back to my original career, electrical engineering. Three years ago, the company I was working for was imploding and the job looked tenuous, so I began to look for other prospects. As I read more about tDCS, I was intrigued. It was hard to imagine something so simple could have so many widespread effects. From an electrical perspective, it is simple: the device supplies low levels (0.5 mA to 2.0 mA) of regulated current through an electrode on the skull (called the “anode” in tDCS), and through the brain; the current then leaves the skull via another electrode (called the “cathode”). I found that the best type of electrode is a sponge electrode, as it provides a better electrical interface and produces less discomfort than other types. I decided to build myself a unit and practice on myself.
The first few times I used the device, I noticed a significant difference in my focus and clarity in all I did the following day. It was like having a strong cup of coffee after not having had coffee in a long time: I was focused, motivated, and had a great problem-solving mind. I also saw it benefit my mood. I decided this was something I wanted to look into further, as I saw first-hand the potential benefits of tDCS for depression.
I became a participator in the Reddit forum on tDCS. Here, people make their own devices, and now more frequently buy the commercial devices supplied by small manufacturers. Many members of this do-it-yourself tDCS community are treating their own depression. Results are remarkable for some of these people, and minimal for others. There are stories of peoples’ lives being changed dramatically within just a few weeks, like coming out of a long lethargy. Other people suffering from multiple conditions – depression, anxiety, and insomnia, for example – may see benefit for only some depression. There appears to be a particularly good success rate with bipolar depression. This is a real-world test of tDCS, outside of the controlled space of research. The results are good overall, but most importantly – with so much chance for unexpected reactions and undesirable side effects – the side effects from the community at large appear similar to what the research shows: slight burning and discomfort at the site during treatment, itching at the site, and a few people get headaches after treatments.
For tDCS, a different position on the head (called “montage”) is like a different remedy with a different intended effect. From a physiological perspective, under the anode, the electrical characteristics at the basement membrane of the neurons are altered (increased potential), making it more likely to fire with neuronal activity. Under the cathode, the potential at the basement membrane is decreased, making the neurons less likely to fire, decreasing neuronal activity. Hence, when you are using tDCS to help learn a new skill (eg, software, writing, language), you practice that skill while you are receiving tDCS, and the neural patterns will form faster than they do during the normal learning process. A typical montage for learning, as well as for depression, is anode to left DorsoLateral PreFrontal Cortex (DLPFC), and cathode to right DLPFC, or Right Supraorbital (see Figure 2).

Figure 2. Left Anodal DLPFC, and Right Cathode Supraorbital Montage
Findings from Clinical Studies
Below are summaries from 3 clinical studies of tDCS for depression, using the anode to left DLPFC montage:
- “The results of this study show that cortical stimulation with tDCS is associated with a significant reduction in depression scores that is specific to the site of stimulation and lasts for at least 30 d after the end of treatment.” (Boggio, 2008)2
- “Although results after 3 weeks of daily tDCS were modest, the number of responders after 6 weeks of treatment was much more encouraging, and comparable with outcomes from a recent large study of 6 weeks of TMS given on an open-label basis to participants with pharmacotherapy-resistant depression. The response rate was superior to that reported for antidepressant medication in individuals who had failed a first course of medication in the large Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study. This suggests that tDCS has meaningful antidepressant efficacy, including in those individuals resistant to pharmacotherapy.” (Loo, 2012)3
- “Continuation tDCS, given weekly for the first 3 months, resulted in the majority of responders remaining well, though the relapse rate increased after treatments were spaced to fortnightly in the subsequent 3 months. In the absence of a control group of responders who did not go on to receive continuation tDCS treatments, we cannot conclude that the continuation treatments were beneficial in preventing relapse, though the higher rate of relapse when treatments were spaced to fortnightly suggests that the weekly treatment schedule may be a useful
treatment strategy.” (Martin, 2012)4
Summary
Direct Current Neurostimulation is still in its early stages. A typical route for medical device development is initially small studies for a particular condition, then larger studies, then FDA involvement. From a regulatory perspective, tDCS devices are not currently regulated as medical devices by the FDA. Commercial manufacturers selling the tDCS device explicitly state that it is not to be used for medical purposes, that it’s not a medical device, etc. However, a lack of involvement by the FDA has allowed thousands of people to try this simple-to-implement but very powerful tool of neuromodulation, and allowed devices that provide this technology to be readily available on the web.
 Keith Spaulding ND, MAc, MSEE, graduated from Bastyr University in 2001. He runs a small company, Human Bioelectric, that designs, develops, and manufactures neurostimulation devices. Its first device, The Cognitive Kit, is a cognitive enhancement device based on transcranial direct current stimulation (tDCS). Keith writes about tDCS when he can to spread the good word, and loves and lives with his family in York, Maine.
Keith Spaulding ND, MAc, MSEE, graduated from Bastyr University in 2001. He runs a small company, Human Bioelectric, that designs, develops, and manufactures neurostimulation devices. Its first device, The Cognitive Kit, is a cognitive enhancement device based on transcranial direct current stimulation (tDCS). Keith writes about tDCS when he can to spread the good word, and loves and lives with his family in York, Maine.
References:
- Nietsch MA, Paulus W. Sustained excitability elevations induced by DC motor cortex stimulation in humans. Neurology. 2001;57(10):1899-1901.
- Boggio PS, Rigonatti SP, Ribeiro RB, et al. A randomized, double-blind clinical trial on the efficacy of cortical direct current stimulation for the treatment of major depression. Int J Neuropsychopharmacol. 2008;11(2):249-254.
- Loo CK, Alonzo A, Martin D, et al. Transcranial direct current stimulation for depression: 3-week randomised, sham-controlled trial. Br J Psychiatry. 2012;200(1):52-59.
- Martin DM, Alonzo A, Ho Ka, et al. Continuation of transcranial direct current stimulation for the prevention of relapse in major depression. J Affect Disord. 2012;144(3):274-278.