

A Very Moldy Story
Joseph Kellerstein, DC, ND
Jennifer is 25 years old and a very philosophically inclined social worker. In fact, she comes from a family whose tradition is discussion and social philosophy, her mother being a university professor. These facts are not obvious when she sits down and beams a very warm, very big soft smile in my direction. Her voice is soft, friendly and makes her seem very mild. Jen is about 5’5” tall with blonde hair and blue eyes. She has no trouble being very open and reflective.
It was mid-November of this year that she presented to the college clinic. It seems the apartment she and her partner were living in had a severe mold problem. The walls were just full of it. Once detected, the problem was addressed, but it rekindled an issue with difficult breathing and severe coughing that was present years ago in childhood (asthma).
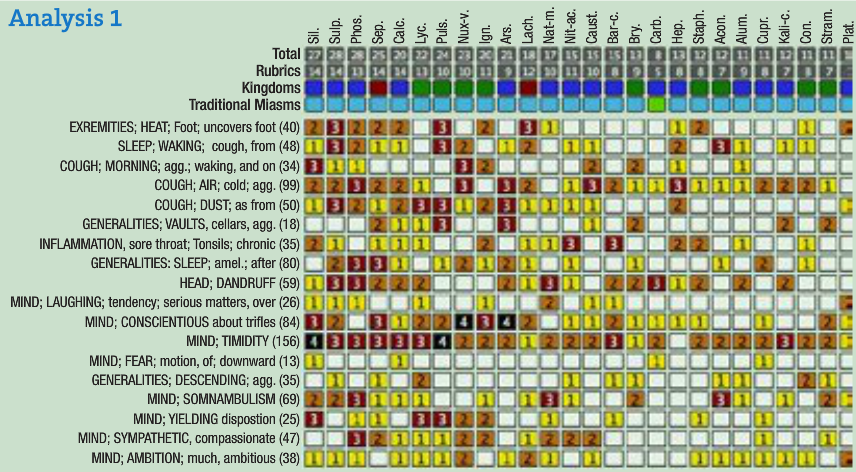
Complaints include asthma, dandruff, throat irritation, and acne. The same familiar triggers were cold air (we have lots of this in Canada in the winter) and vacuuming. As a child, it was typical to wake herself from coughing. She is experiencing this again now. She will cough a lot at night but it seems far less intense after rising.
Jen has a history of chronic tonsillitis. Throat pain is still the hallmark of illness for her. ”Whenever I get sick, first there is a sore throat.” The only modality I could get was “it is better if I sleep a lot.”
There was use of oral contraceptives from 18-22 years of age. “When I stopped, up came acne. It was worse along the jawline and worse before menses.”
There were a few years where she would clench at night and then wake with a headache. A past symptom.
She is presently working very hard on her dissertation. “I have stepped down from responsibility at work. Sometimes when I work I feel as if I am wasting time.” Energy has certainly been affected by this malady, but not in any characteristic way. With this fatigue it is harder to “force myself” to go to yoga.
Jennifer is vegan.
“I can get very anxious if I feel I have disappointed someone. I am very sensitive to conflict.” When anxious, her back muscles get sore and her body heats up. When prompted by this idea of heat I dove into a detailed thermal profile and came up with the fact that she will always sleep with her feet out because they are so hot.
Jennifer has strong academic ambitions and is quite perfectionistic. She is not stubborn and in personal issues tends to give in. She is quite attuned to the feelings of others in proximity and to social issues. However despite the obvious sweet and mild manner, the sympathy has an analytical tinge. There is a history (past) of sleep walking and a fear of downward motion (escalators, etc).
Objectively I notice the smiles get larger and more intense when discussing something stressful like the breathing.
Those smiles broadening so much when speaking of difficulty caught my attention. I know from training and experience that these objective signs can be very guiding in remedial selection.
Her feet always being hot at night and requiring uncovering is also a good symptom. To me, these 2 symptoms plus her intense intellectual state (to the point of other duties feel like a waste of time) to some degree characterize the person.
There was not a whole lot to characterize the disease. Given these facts I opted to begin the case with Sulphur.
This is a lady with strong environmental sensitivities related to breathing, so I was concerned about potency. The prescription was Sulphur 6C,1 pellet once a week.
First Follow-Up
The first follow up was early January.
The cough is much less. She had been bicycling in the cold and breathing was less troublesome. Overall there is a far diminished frequency of difficult respiration. Sleep has improved because she is no longer waking with the cough.
Recent Follow-Up
The most recent follow up was mid-February.
The breathing has been completely better. There have been no throat issues (now my case-taking here was incomplete – I did not note that the throat was painful at least half the time. However it was a pleasant correction.)
Jennifer notices the dandruff (and I wonder about the acne) seems proportional to sugar intake. (When people are trained to self-observe by participation in this homeopathic process, a heightened, often useful self-observation occurs relative to hygienic influence.)
Jennifer also notices that her feet are sticking out of the covers again (I did not know that had changed!) I took this to be the early signs of a relapse and increased the potency to a 30C once per week.
At this point the case is not yet fully cured because the acne and dandruff persist.
Comments
This simple case demonstrates the ability of homeopathy to cut through much detail to the facts that will influence the body in healing itself under remedial stimulus. We have a demonstration of the importance of objective symptoms. The foot symptom shows the importance of keynotes and using the relapse of these symptoms of the person (not necessarily the illness) as a guide in prescribing and adjustment of potency.
Homeopathy provides us a very rich literature of cure and clinical wisdom that dates back to Hahnemann. It is a body of knowledge confirmed in the experience of many fine Hahnemannians over 200 years. We continue to daily verify the accuracy and wisdom of these pioneers today in practice.
The naturopathic profession has had a fantastic record of excellence in homeopathic training. Naturopaths are leading the world in finally continuing the work of the great pioneers of this field in amassing and organizing existing data so as to advance our knowledge of pure materia medica and the completeness of the repertory. This is work that homeopathy has neglected for over a century.
Over the last decade it seems that some very “innovative” uses of homeopathic remedies based on the teachings of charismatic seminar leaders have become popular in certain schools. These newer teachings arguably are not homeopathic. They have a deductive basis. Homeopathy is inductive. I do not argue their efficacy because I choose to practice Homeopathy and so cannot comment.
It seems to me that our institutions are there to provide excellence at basics. Why is it in this instance that some operate as if they were a franchise for speakers on the seminar circuit? At the very least, this study should be distinguished from homeopathy and called something else to minimize academic confusion.
The net effect is that my colleagues (so educated) are homeopathically illiterate. They are unable to work with 200 years of homeopathic literature and the thousands of cured cases because they lack competence in foundational knowledge and clinical skills needed for the practice of homeopathy. Many have little knowledge of first aid remedies, basic case taking and repertory skills, and certainly a tiny knowledge of Pure Materia Medica.
The purpose of my writing these cases is to show that homeopathy is not nebulous, cultish or a pseudo religious pursuit, but simply a rational medicine based on observation and a wonderful 200-year-old tradition of honest investigation.
 Joe Kellerstein, DC, ND graduated as a chiropractor in 1980 and as an ND in 1984. He graduated with a specialty in homeopathy from the Canadian Academy for Homeopathy, and subsequently lectured there for two years. He also lectured in homeopathy for several years at CCNM; for eight years at the Toronto School of Homeopathic Medicine; and for two years at the British Institute for Homeopathy. Dr. Kellerstein’s mission is the exploration of natural medicine in a holistic context, especially homeopathy and facilitating the experience of healing in clients.
Joe Kellerstein, DC, ND graduated as a chiropractor in 1980 and as an ND in 1984. He graduated with a specialty in homeopathy from the Canadian Academy for Homeopathy, and subsequently lectured there for two years. He also lectured in homeopathy for several years at CCNM; for eight years at the Toronto School of Homeopathic Medicine; and for two years at the British Institute for Homeopathy. Dr. Kellerstein’s mission is the exploration of natural medicine in a holistic context, especially homeopathy and facilitating the experience of healing in clients.






{kind=link}