
Donna Beck, ND
“I just don’t understand it, Doctor. I’m not like my other friends. They all seem to be thriving on gluten-free diets or the Mediterranean diet or the Paleo diet – not me! Wheat and gluten products don’t bother me at all. In fact, it seems to be one of the things I thrive on. My most severe reactions are to olive and coconut oil. You know how everyone loves their olive and coconut oil these days. It seems to be in everything! It’s almost impossible to eat out, as most restaurants cook with olive oil. The first time I reacted to it was when I was eating potato chips made in olive oil. I actually got lightheaded to the point of passing out. My blood pressure dropped. I experienced a scary sensation of not being able to get a deep breath. It went on for over an hour, gradually subsiding.Ms B sat across from me, looking very frustrated…
“I have had this same reaction with other foods. The worst reaction I ever had was when I ate my friend’s homemade honey/blueberry/black currant jam. I thought I was having a panic attack and almost went to the hospital, but it slowly passed. Another less scary but annoying symptom is hives all over my torso. It always seems to be at the end of every day now.
“I also noticed that I get up about every hour or two during the night to urinate. I try not to drink a lot of liquid past 5 PM, but I often feel thirsty and dehydrated. I feel constipated and gassy most of the time. I haven’t had any of those severe reactions again, but when I filled out the diet and symptom diary as you recommended, I noticed that I have lesser but similar reactions to cucumbers, some steamed greens, and various herbs and spices. Curry, chili, paprika, black pepper, and turmeric seem to be the worst. Now I am finding turmeric everywhere in supplements, so I have to read labels carefully. I am being very careful to avoid the things I know I react to, but I still feel very unwell most of the time. What could be going on, Doc? I don’t know what to eat anymore.”
Using as a clue the blueberry/currant/honey jam episode provided by Ms B, I discovered that the common factor among her reactive foods was high salicylate content. A closer look at her diet diary showed that she was drinking 8–10 oz of almond milk daily. To avoid olive and coconut oil, she was cooking with walnut and avocado oil – also moderately high in salicylates. Her supplement regimen included several nutrient/herbal combinations. Even with her avoidance of turmeric, she was supplementing daily with herbal extracts and “plant-based nutrients,” which were actually another concentrated source of salicylates. All “tolled,” Ms B was on a very high-salicylate diet and supplement regimen. The fact that grains and meat are very low in salicylates helped confirm my suspicions about her salicylate reactions, as she reported having no problems with most meats or gluten-based grains. In fact, these foods, along with Brassica family vegetables (also low in salicylates), had become her mainstay.
Although this type of food intolerance may not be currently “trending” with Ms B’s friends, salicylate intolerance is not unknown in the medical literature. Benjamin F. Feingold, MD, is probably the most widely known person to study this chemical and develop what is now referred to as the “Feingold Diet.” Parents with children on the Autism Spectrum are usually familiar with his work. He started out in the 1960s as a pediatrician and allergist, studying children’s negative reactions to aspirin.1 Another pioneer in identifying salicylate problems is allergy researcher, Anne R. Swain, PhD, of Sydney, Australia. Dr Swain carried out experiments between 1977 and 1986, quantifying the salicylate content of many foods and noting reactions in test subjects. Her thesis, “The Role of Natural Salicylates in Food Intolerances,” became a definitive work, launching others to do further study on salicylate reactions.2
In Swain’s tables listing salicylate content of common foods, one sees that blueberries contain 2.76 mg of salicylates per 100 grams. Black and red currants contain 3.06-5.06 mg of salicylates per 100 grams. Honey’s salicylate content ranges from 2.5 to 11.24 mg/100 grams. Ms B’s jam was made with dried currants that had been boiled and strained. Drying fruit increases the salicylate content; boiling and reducing the syrup from the dried currants concentrates it further. The fresh blueberry-dried currant mixture was further mixed and reduced along with honey, making the concentration of salicylates in this homemade jam unknown without testing it in a lab. However, it is easy to extrapolate from these tables that Ms B’s jam had a very high salicylate content.2,3 Further, in Swain’s article it is stated that “some of the herbs and spices [tested] contain much more salicylate than has previously been reported for any food. We found that curry powder contains 218 mg salicylate per 100 g. Others almost as high were paprika, thyme, dill powder, garam masala, oregano, and turmeric.”2-4
What are Salicylates?
Salicylates are the salts and esters of salicylic acid. Naturally occurring in varying concentrations in many fruits and vegetables, salicylates are stored in the bark, leaves, roots, and seeds of plants, and act as a natural immune hormone and preservative, preventing rotting and protecting the plant against harmful insects, bacteria, and fungi. Salicylates are chemically very similar to the man-made chemical, acetylsalicylic acid, a key ingredient in aspirin and other pain medications. They are also frequently found in cosmetics and personal care products.5
Common products containing salicylates include:
- acne and wart removal products, aspirin, many NSAIDs, and other medications, both natural and pharmaceutical
- herbal products
- cosmetics, fragrances, perfumes, lotions, hair spray, gels, shampoo and conditioners, bubble baths
- cleaning products
- air fresheners
- gums and breath savers, lozenges
Of particular interest is the increased use of salicylates in agricultural practice. The “Report of the New York State College of Agriculture,” regarding the use of salicylates in food preservation, states, “Salicylic acid and the salicylates added to foods even in small quantities exert a depressing and harmful influence on digestion and health and upon the metabolic activities of the body.”6 It is also now known that plants produce more salicylic acid when they are stressed.7 This fact is being used purposefully in agriculture to stimulate blooming times in plants and to enhance crop yield.8 However useful this could be in feeding an environmentally stressed planet, this new practice in agriculture, combined with the natural increase in salicylates in stressed plants, could greatly increase the amount of salicylic acid consumed in the average diet.
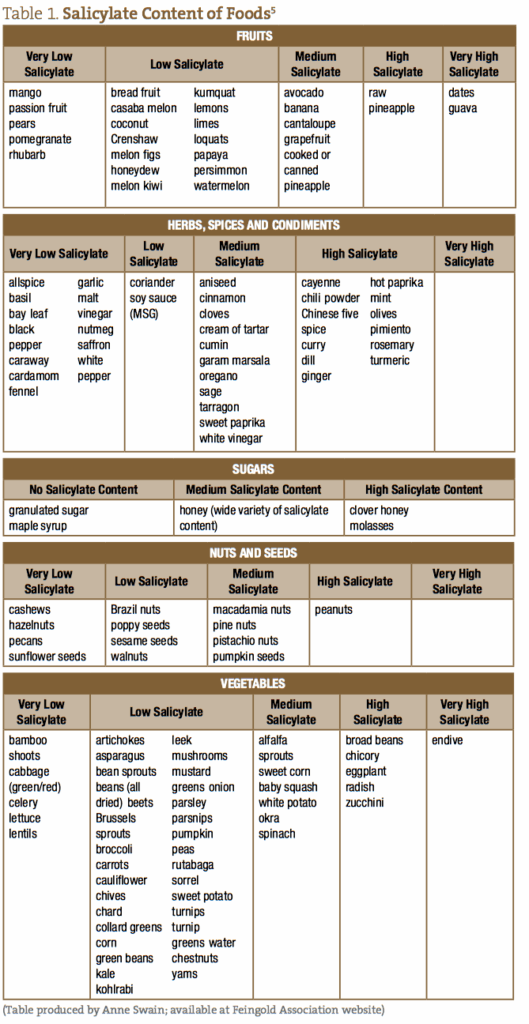
See Table 1 for Anne Swain’s partial list of salicylate–containing foods and foodstuffs.5
Salicylate Toxicity
Ms B’s symptoms were consistent with the pattern of physiological change that occurs when the body shifts to a state of metabolic acidosis. She began to hyperventilate due to the increased pH in her digestive system. Hyperventilation serves to automatically restore balance (homeostasis) to the body’s chemistry, since it lowers carbon dioxide in the body, which buffers an excess of acid in the blood. Ms B was not an aspirin user; however, her diet contained enough aspirin–like compounds that she had symptoms mimicking aspirin toxicity.
Much variability occurs among individuals who have developed salicylate intolerance, from symptoms of low-grade chronic toxicity, to acutely flaring toxicity reactions.9 Once again referencing Dr Swain’s research, people with salicylate intolerances show symptoms at very low concentrations of salicylate ingestion, sometimes as low as 35 mg/100 g of salicylate–containing foods or substances.2 Asthma, eczema, rhinitis, sinus irritation, conjunctivitis, stomach ache, and irritable bowel are among the most common symptoms of salicylate intolerance. Other symptoms include hives, migraines, and hyperactivity in children.10
It is safe to assume that people who suffer salicylate sensitivity would be more susceptible to acute salicylate toxicity. Toxicity occurs when the body’s acid buffering systems are overloaded and overwhelmed. These symptoms are the same as in aspirin poisoning: nausea, vomiting, diaphoresis, and tinnitus are the earliest signs and symptoms of aspirin poisoning. Other early symptoms and signs can include vertigo, hyperventilation, tachycardia, and hyperactivity. As toxicity progresses, agitation, delirium, hallucinations, convulsions, lethargy, and stupor may occur. Hyperthermia is an indication of severe toxicity, especially in young children.11 Note: Chronic toxicity can develop from doses of aspirin at 100 mg/kg/day in people without salicylate sensitivity.9
Phases of Salicylate Toxicity
The acid/-base, fluid, and electrolyte abnormalities seen with salicylate toxicity can be grouped into 3 phases12:
Phase 1 is characterized by hyperventilation resulting from direct respiratory center stimulation. This leads to respiratory alkalosis and compensatory alkaluria. Potassium and sodium bicarbonate are excreted in the urine. This phase may last as long as 12 hours.
In phase 2, paradoxical aciduria in the presence of continued respiratory alkalosis occurs when sufficient potassium has been lost from the kidneys. This phase may begin within hours and last 12–24 hours.
Phase 3 includes dehydration, hypokalemia, and progressive metabolic acidosis. This phase may begin 4-6 hours after ingestion in a young infant, or 24 hours or more after ingestion in an adolescent or adult.13
Salicylate Metabolism
Salicylates are readily absorbed in the un-ionized form from the small intestine. They distribute rapidly into the body’s fluid compartments and bind to albumin in the plasma. The unbound fraction increases as total plasma salicylate concentrations increase. The major route of biotransformation is hepatic conjugation with glycine in the liver.14 This occurs primarily with glycine or glucuronic acid, involving different metabolic pathways. The main pathway, glycine conjugation, is saturable. With low doses of aspirin (or other salicylate sources), approximately 90% of salicylate is metabolized through this pathway. As this major pathway maxes out, the secondary pathways become more important.14
Therefore, the half–life of salicylate depends on the major metabolic pathway used at a given concentration, and becomes longer with increasing dosage. Salicylate is said to follow nonlinear kinetics at the upper limit of the dosing range.15,16 Studies have shown that there is much inter-subject variation with respect to the relative contribution of the different salicylate metabolic pathways. Urinary excretion of unchanged salicylate accounts for 10% of the total elimination of salicylate. Excretion of salicylate results in glomerular filtration, with active proximal tubular secretion through the organic acid transporters and passive tubular reabsorption. Urinary excretion is markedly pH-dependent, and as the urinary pH rises from 5 to 8, the amount of excreted free ionized salicylate increases from 3% of the total salicylate dose to more than 80% (by ion trappings in the urine). Therefore, the amount of salicylates excreted via the urine is markedly increased when the urine is alkaline.15,16
In other words, the more acidic the urine becomes from the presence of salicylates, the more salicylates are held in the body. A build-up occurs, causing more even acidity; a vicious cycle ensues. High levels of salicylate are toxic because the drug uncouples oxidative phosphorylation, as well as inhibiting some enzymes in the cell.15,16
In normal metabolism, ie, with correct levels of sulfates and liver enzymes, phenols and salicylates are easily metabolized. The body utilizes what it needs from the chemicals and properly disposes of the rest through the bowels. In those whose sulfate and liver enzyme levels are abnormal, or in the case of leaky gut syndrome, intolerance to this chemical family can occur rather quickly.17 Research by Dr Rosemary Waring at the University of Birmingham found that children on the Autism Spectrum have low levels of the enzyme phenolsulfotransferase-P.18 This enzyme breaks down phenols such as salicylates, as well as amine family substances. Without normal levels of phenolsulfotransferase-P, and the substrate it uses, sulfates, the sulfotransferase enzyme cannot do the task it was created to do, ie, metabolize salicylates. The end result is salicylate intolerance and the subsequent physical and behavioral reactions that come with it.18
Ms B – Follow-up
With assistance from charts identifying foods low in salicylates,4 Ms B was put on a no/low-salicylate-free diet for 2 weeks. At her follow-up visit, she reported a “medical miracle.” Her hives were gone. She had more energy, as she was sleeping better at night. She no longer had to get up to urinate every 2 hours. Her lifelong constipation had disappeared, along with the daily gassy feeling she reported. Best of all, she felt like she could catch her breath again.
The future treatment plan for Ms B was to include further exploration as to why she might have developed salicylate sensitivity. Other important aspects of her medical history included recent menopause and an injury to her cervical spine. These 2 events likely increased overall inflammation in her system, as well as presented a challenge to her adrenal glands, potentially disrupting cortisol levels. For now, she was to continue her low-salicylate diet.
Useful Considerations
Many people who are under chronic stress develop gut issues, such as yeast/bacterial overgrowth, or digestive diseases. This may lead to the development of salicylate and other intolerances, as a result of leaky gut. Low-salicylate- and salicylate–free diets, as well as diet regimens such as the Specific Carbohydrate Diet, may be useful.17 After eliminating the organisms that cause the dysbiosis, care must be taken to rebuild a healthy gut lining. Certain amino acids, such as arginine, lysine, serine, glycine, alanine, choline, tyrosine, phenylalanine, tryptophan, carnitine, and taurine may be especially useful. Some helpful nutrients which are likely to be salicylate-free include: Vitamins A, C (without bioflavonoids), E, D, B-complex, beta-carotene, B6, folate, and inositol hexanicotinate. Foods such as sauerkraut are no-salicylate and contribute healthy short-chain fatty acids to the colonic environment.
Supplementation to support sulfation pathways in the body also should also improve tolerance. This approach is something that should be considered if improvements are seen by eliminating the salicylate-rich foods.19 Supportive substances include: glutathione, alpha-lipoic acid, N-acetylcysteine, and methylsulfonylmethane (MSM).
Take into account patients vulnerable to salicylate intolerance who already use daily aspirin for its blood-thinning effect, also patients with liver or kidney impairment. These patients may need to find alternative, low-salicylate blood thinners. This could include garlic or no/low-salicylate pharmaceuticals. Other vulnerable patients include those with heavy metal toxicity, the elderly, and children with Autism Spectrum disorders.
With the current focus on gluten sensitivity in marketing and social media, salicylate intolerance is an overlooked source of allergic reactions. There are likely numerous patients like Ms B who have developed salicylate sensitivity over time, perhaps partly due to the rising amounts of salicylates used in foods and consumer products. For this reason, salicylate sensitivity should be on the watchlist, as it is likely to gain popularity as the “other food intolerance.”
 Donna Beck, ND, graduated from NCNM in Portland, OR, in 1992, after which she completed a 2-year family residency at NCNM’s teaching clinic. Dr Beck has maintained a private practice – A Family Wellness Center – in Gresham, OR, for over 20 years. Although she treats many common and chronic health conditions, she has a special interest in digestive problems, allergies, and endocrine imbalances. For over 15 years, Dr Beck has also taught students of natural medicine. For many years, Dr Beck worked as an attending physician in NCNM’s teaching clinic. She served for 3 years on the board of directors at NCNM as Chair of the Academic Affairs Committee; she also served on the Oregon Board of Naturopathic Medicine.
Donna Beck, ND, graduated from NCNM in Portland, OR, in 1992, after which she completed a 2-year family residency at NCNM’s teaching clinic. Dr Beck has maintained a private practice – A Family Wellness Center – in Gresham, OR, for over 20 years. Although she treats many common and chronic health conditions, she has a special interest in digestive problems, allergies, and endocrine imbalances. For over 15 years, Dr Beck has also taught students of natural medicine. For many years, Dr Beck worked as an attending physician in NCNM’s teaching clinic. She served for 3 years on the board of directors at NCNM as Chair of the Academic Affairs Committee; she also served on the Oregon Board of Naturopathic Medicine.
References
- Edulkind S, ed. Feingold Bluebook. 2012. Feingold Association of the U.S. Available at: http://www.feingold.org/BLUEBOOK.pdf. Accessed November 15, 2015.
- Swain AR, Dutton SP, Truswell AS. Salicylates in foods. J Am Diet Assoc. Human Nutrition Unit. 1985;85(8):950-960. Available at: http://www.slhd.nsw.gov.au/rpa/allergy/research/salicylatesinfoods.pdf. Accessed December 15, 20156.
- Swain AR. The role of natural salicylates in food intolerance. [PhD thesis; University of Sydney] 1988. Available at: http://www.slhd.nsw.gov.au/rpa/allergy/research/students/1988/anneswainphdthesis.pdf . Accessed December 15, 2015.
- SalicylateSensitivity:FoodGuide. Available at:http://salicylatesensitivity.com/about/food-guide/. Accessed November 15, 2015.
- Swain AR. Salicylate list. Feingold Association Web site. http://www.feingold.org/DOCS/SalicylateList.pdf. Accessed November 15, 2015.
- New York State College of Agriculture. Twenty-Fifth Annual Report of the New York State College of Agriculture at Cornell University and the Agricultural Experiment Station. Ithaca, NY: J. B. Lyon Company; 1913. Page available at: http://tinyurl.com/jt67oam. Accessed November 15, 2015.
- Karl T, Guenther A, Turnipseed A, et al. Plants in forest emit aspirin chemical to deal with stress: Discovery many help agriculture. September 8, 2008. AtmosNews. NCAR/UCAR Web site. https://www2.ucar.edu/atmosnews/news/921/plants-forest-emit-aspirin-chemical-deal-stress-discovery-may-help-agriculture. Accessed November 15, 2015.
- Karlidag H, Yildirim E, Turan M. Exogenous applications of salicylic acid affect quality and yield of strawberry grown under antifrost heated greenhouse conditions. J Plant Nutr Soil Sci. 2009;172(2):270-276.
- Salicylates. Open Source Clinical Toxicology Curriculum. Wiki Tox Web site. http://curriculum.toxicology.wikispaces.net/2.1.1.4+Salicylates. Accessed November 15, 2015.
- Feingold Association. Salicylate & Aspirin Sensitivity. Available at: http://www.feingold.org/sas.html. Accessed November 15, 2015.
- Meves A, Stock SN, Beyerle A, et al. Vitamin C derivative ascorbyl palmitate promotes ultravioletBinduced lipid peroxidation and cytotoxicity in keratinocytes. J Invest Dermatol. 2002;119(5):11031108.
- Waseem M. Salicylate Toxicity. December 5, 2015. Medscape, Drugs and Diseases. Available at: http://emedicine.medscape.com/article/1009987-overview. Accessed December 15, 2015.
- Mancini MC. Pediatric respiratory alkalosis. Updated January 16, 2015. Medscape, Drugs & Diseases. Available at: http://emedicine.medscape.com/article/906929-overview. Accessed December 15, 2015.
- Aspirin Pharmacokinetics. Université de Lausanne. UNIL Web site. http://sepia.unil.ch/pharmacology/index.php?id=83. Accessed November 15, 2015.
- Brandis K. Metabolic Acidosis due to Drugs and Toxins. AcidBase Physiology. In: The Physiology Viva: Questions & Answers. Oxenford, Queensland: Alderbury House Publishing; 1997. Available at: http://www.anaesthesiamcq.com/AcidBaseBook/ab8_6c.php. Accessed November 15, 2015.
- Pharmacokinetics: Renal Excretion. Université de Lausanne. UNIL Web site. http://sepia.unil.ch/pharmacology/index.php?id=58. Accessed November 15, 2015.
- Reasoner J. Leaky Gut Syndrome in Plain English – and How to Fix It. SCD Lifestyle Web site. http://scdlifestyle.com/2010/03/the-scd-diet-and-leaky-gut-syndrome/. Accessed November 15, 2015.
- O’Reilly BA, Waring RH. Enzyme and sulphur oxidation deficiencies in autistic children with known food/chemical intolerances. J Orthomol Med. 1993;8(4):198-200. Available at: http://www.orthomolecular.org/library/jom/1993/pdf/1993-v08n04-p198.pdf.
- Salicylates (Feingold Diet). The healing touch therapy Web site. http://www.thehealingtouchtherapy.co.uk/contentextra.asp?ContentId=12. Accessed November 15, 2015











