Dugald Seely, ND
Naturopathic doctors are well placed to offer high-quality, holistic care to cancer patients. There’s no debate that cancer treatment can be daunting and difficult with respect to both therapy and emotional involvement, yet, as clinicians we can provide real benefit to patient quality of life and potentially to their quantity of life as well. Much more clinical research needs to be done; however, there is a growing body of evidence to support a myriad of treatments NDs have to offer in cancer care.
Complementary and integrative therapies available to NDs in the fight against cancer are extensive and provide one of our greatest strengths. With our eclectic approach we can individualize treatment and, perhaps more importantly, go after cancer from a number of angles. The ability to put together treatment regimens that are synergistic and intelligently thought out is a luxury that oncologists do not share to anywhere near the same degree. Surgery, chemotherapy and radiation therapy are important first-line therapeutic tools, yet there are more options … ones readily available and at our disposal.
My goal in this article is to briefly elucidate the mechanisms of cancer progression that provide the most vulnerable targets for the kinds of therapies we use. The concept I would like to put forward most is the idea that metastasis is an inherently inefficient process and one that requires a number of cellular traits to be in place for it to successfully occur. Some of the characteristics necessary for this process include achieving the total combination of the following abnormal cellular attributes (Gupta and Massague, 2006; Gupta et al., 2007):
- Resistance to extracellular and intracellular death signals
- Increased motility
- Ability to break down the basement membrane and extracellular matrix
- Ability to intravasate
- Ability to survive transport within blood circulation or through the lymph
- Ability to evade the immune system
- Ability to extravasate
- Ability to co-opt local, non-cancerous stromal cells
- Ability to promote angiogenesis
- Ability to be indefinitely selfproliferative.
These characteristics are essential for any cell or group of cells to acquire in order to become metastatic. Certain cancers, including pediatric blood-borne cancers, may already have some of these abilities inherently, but the vast majority of cancers initially start with none of these physiological abilities intact. The clinical significance is that without metastasis cancer would be far less deadly than it is. In fact, 90% of cancer mortality arises as a result of metastasis (Mehlen and Puisieux, 2006). What is truly relevant is that cells are being constantly shed by tumors; however, very few of them are able to produce a successful micro-metastasis downstream of the primary tumor. Model systems in the lab and in vivo indicate that one million cancer cells per gram of tumor tissue can be seeded into the bloodstream daily (Chang et al., 2000). The vast majority of these cells, however, are unable to successfully metastasize. This is an important reality, for if we are able to augment any of the barriers and make it harder for metastasis to occur, can we not then further decrease an already low probability of cancer spread? Theoretically, I think the answer is a resounding yes, and while the research base is limited, the idea is gaining support from the evidence.
 Molecular Agents
Molecular Agents
Conventional chemotherapy, while not abandoning older, highly cytotoxic drugs, is moving towards the use of newer molecular agents that target cellular mechanisms inherent and ideally specific to cancer cells. Successful examples of these agents include bevacizumab and trastuzumab. Bevacizumab is a VEGF monoclonal antibody that targets the development of angiogenesis, thereby depriving cancer tissue of needed nutrients and oxygen as well as reducing the likelihood of spread (Shih and Lindley, 2006). Trastuzumab is also a monoclonal antibody targeted against the HER2 onco-protein overexpressed in 25% of all breast cancers and that has been associated clearly with poor prognosis (Tsakonas and Kosmas, 2007).
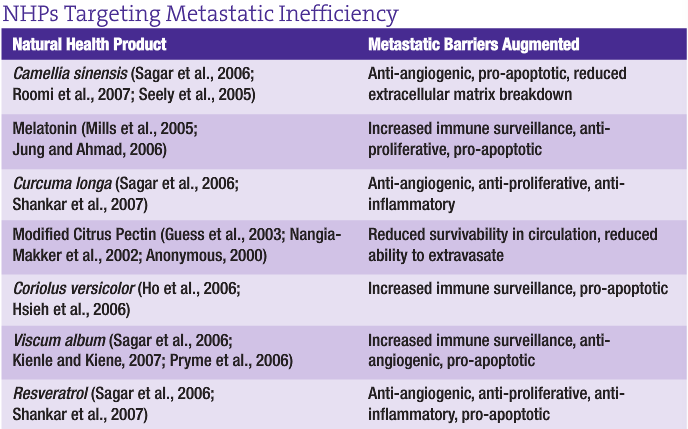
The idea behind these newer biologic agents is that by targeting molecular pathways critical to cancer progression, cancer can be better managed. Indeed, the idea of managing cancer as a chronic condition rather than attempting to cure it is gaining in stature. Some benefits are being achieved; however, conventional therapies are still limited to the pharmaceutical model, which largely employs a mono-therapeutic approach. In addition to a number of other therapies, NDs have access to a wide selection of natural health products (NHPs) and other complementary therapies that can act on the processes required for metastatic spread from many angles simultaneously. A small fraction of examples of promising NHPs are provided in Table 1 that target the cellular mechanisms that ultimately drive cancer and its metastatic spread. Synergy is our ally in this fight. If we can enhance metastatic inefficiency via a ‘holistic’ cell-based treatment, then we may indeed help control cancer progression.
Through the augmentation of barriers to metastasis, I believe an effective anti-cancer management approach is within the ND’s grasp via an extensive therapeutic toolkit. Numerous NHPs have demonstrated evidence of being able to act at different levels within the metastatic pathway. Combining NHPs to target these metastatic barriers should theoretically create an anti-metastatic environment within the body without concomitant cytotoxicity. Our materia medica is rife with examples of these kinds of NHPs. Table 1 provides just a small selection of some of those that show real promise.
Of course, the devil is in the details, and knowing one’s therapies well is critical to filling a quiver of therapeutic options. Recent articles from the February issue of NDNR, including Dr. Uzick’s elucidation of flax for breast cancer and Drs. Yarnell and Russel’s discussion of botanical options for cervical dysplasia, provide exactly the kind of information needed to build well-informed clinical trust in specific therapeutic choices. Treatment can and should be applied with the idea of enhancing the body’s own innate ability to hinder the spread of cancer. The strategic approach to augmenting our own body’s innate defenses against metastasis is fully in line with our philosophy and the Vis. Other therapeutic options should be considered within this context and seen as a way of adding to the body’s overall capacity to get rid of cancer on its own terms. Whether it is the use of modified citrus pectin to isolate cancer cells in circulation; the use of hydrotherapy to increase immune surveillance; or the use of intravenous vitamin C to increase cancer cell apoptosis; the end goals remain the same: eradication of malignant cells and support of innate defenses. Medical oncologists have the former approach down pat, and I think a good case can be made that we typically have focused on the latter. The two together, however, provide a powerful combination.
 It probably should come as no surprise that new treatments in conventional cancer therapy are working to target aspects of cancer progression that so many of our own treatments already exhibit. The experience being built by ND clinicians and the evidence for specific natural agents and especially the combination of treatments in cancer research is growing. As our level of understanding and development of treatment options become more sophisticated, we can and will make great progress in our ability to control and manage cancer.
It probably should come as no surprise that new treatments in conventional cancer therapy are working to target aspects of cancer progression that so many of our own treatments already exhibit. The experience being built by ND clinicians and the evidence for specific natural agents and especially the combination of treatments in cancer research is growing. As our level of understanding and development of treatment options become more sophisticated, we can and will make great progress in our ability to control and manage cancer.
 Dugald Seely ND, MSc is director of research at CCNM and editor-in-chief for the soon to be re-launched International Journal of Naturopathic Medicine. At the Toronto naturopathic college, Dr. Seely is involved in the conduct and supervision of research on naturopathic therapies, with a primary focus in the area of cancer research. Dr. Seely is keen on building external collaborative links with other researchers and clinicians, and is active in a number of research networks. He has published numerous peer-reviewed papers and is a frequent speaker at national and international conferences. As a clinician, Dr. Seely runs a small practicefocused on the treatment of patients with cancer or wishing to prevent cancer.
Dugald Seely ND, MSc is director of research at CCNM and editor-in-chief for the soon to be re-launched International Journal of Naturopathic Medicine. At the Toronto naturopathic college, Dr. Seely is involved in the conduct and supervision of research on naturopathic therapies, with a primary focus in the area of cancer research. Dr. Seely is keen on building external collaborative links with other researchers and clinicians, and is active in a number of research networks. He has published numerous peer-reviewed papers and is a frequent speaker at national and international conferences. As a clinician, Dr. Seely runs a small practicefocused on the treatment of patients with cancer or wishing to prevent cancer.
References
Gupta GP and Massague J: Cancer metastasis: building a framework, Cell Nov 17;127(4):679-95, 2006.
Gupta GP et al: Mediators of vascular remodelling coopted for sequential steps in lung metastasis, Nature Apr 12;446(7137):765-70, 2007.
Mehlen P and Puisieux A: Metastasis: a question of life or death, Nat Rev Cancer Jun;6(6):449-58, 2006.
Chang YS et al: Mosaic blood vessels in tumors: frequency of cancer cells in contact with flowing blood, Proc Natl Acad Sci USA Dec 19;97(26):14608-13, 2000.
Shih T and Lindley C: Bevacizumab: an angiogenesis inhibitor for the treatment of solid malignancies, Clinical Therapeutics Nov;28(11):1779-802, 2006.
Tsakonas G and Kosmas C: Integration of novel targeted therapies into the systemic treatment of breast cancer – a review, J Buon Jul-Sep;12(3):319-27, 2007.
Sagar SM et al: Natural health products that inhibit angiogenesis: a potential source for investigational new agents to treat cancer – part 1, Current Oncology Feb;13(1):14-26, 2006.
Roomi MW et al: Inhibition of cell invasion and MMP production by a nutrient mixture in malignant liposarcoma cell line SW-872, Medical Oncology 24(4):394-401, 2007.
Seely D et al: The effects of green tea consumption on incidence of breast cancer and recurrence of breast cancer: a systematic review and meta-analysis, Integrative Cancer Therapies Jun;4(2):144-55, 2005.
Mills E et al: Melatonin in the treatment of cancer: a systematic review of randomized controlled trials and meta-analysis, Journal of Pineal Research Nov;39(4):360-6, 2005.
Jung B and Ahmad N: Melatonin in cancer management: progress and promise, Cancer Research Oct 15;66(20):9789-93, 2006.
Shankar S et al: Curcumin enhances the apoptosis-inducing potential of TRAIL in prostate cancer cells: molecular mechanisms of apoptosis, migration and angiogenesis, J Mol Signal Oct 4;2(1):10, 2007.
Guess BW et al: Modified citrus pectin (MCP) increases the prostate-specific antigen doubling time in men with prostate cancer: a phase II pilot study, Prostate Cancer and Prostatic Diseases 6(4):301-4, 2003.
Nangia-Makker P et al: Inhibition of human cancer cell growth and metastasis in nude mice by oral intake of modified citrus pectin, Journal of the National Cancer Institute Dec 18;94(24):1854-62, 2002.
Anonymous: Modified citrus pectin-monograph, Altern Med Rev Dec;5(6):573-5, 2000.
Ho CY et al: Coriolus versicolor (Yunzhi) extract attenuates growth of human leukemia xenografts and induces apoptosis through the mitochondrial pathway, Oncology Reports Sep;16(3):609-16, 2006.
Hsieh TC et al: Induction of cell cycle changes and modulation of apoptogenic/anti-apoptotic and extracellular signaling regulatory protein expression by water extracts of I’m-Yunity (PSP), BMC Complementary and Alternative Medicine 6:30, 2006.
Kienle GS and Kiene H: Complementary cancer therapy: a systematic review of prospective clinical trials on anthroposophic mistletoe extracts, European Journal of Medical Research Mar 26;12(3):103-19, 2007.
Pryme IF et al: Suppression of growth of tumour cell lines in vitro and tumours in vivo by mistletoe lectins, Histology and Histopathology Mar;21(3):285-99, 2006.
Shankar S et al: Chemoprevention by resveratrol: molecular mechanisms and therapeutic potential, Front Biosci
12:4839-54, 2007.