

Notes from the Field: May, 2021
JARED L. ZEFF, ND, VNMI, LAC
The following is not an article prepared for a medical journal. Not every statement of fact is cited or referenced. This is a commentary on the medicine, a running set of observations about practice in the field. It’s not meant to be a peer-reviewed presentation; rather, these are notes and thoughts from a practicing naturopathic physician, a primary care doc in general practice.
Finding The Cause (Part II)
In my last article on this subject, I emphasized toxemia as a major cause of disease. In this second part, I want to explore some additional elements to consider and tools to use when seeking cause. When contemplating why people become sick, modern medicine readily presents an answer – they have acquired or developed some type of pathology or disease. They have cancer, arthritis, multiple sclerosis, or influenza, etc. That is why they are ill. There are diagnostic algorithms to diagnose the specific disease entity, and there are prescribed treatments, hopefully, to treat the disease, so that they can recover. It makes logical sense that by seeking the cause of a disease, the resulting illness could be addressed. What if, however, we were to look at the cause of illness itself, rather than the cause of a specific disease? What diagnostic approaches then become available, what treatments? One local doctor addressed this philosophical difference when he told one of my patients, “Do not plan on being cured. We do not do that. We manage your disease.” To this doctor, illness was defined as the resulting experience of a disease, and in searching for cause and eventual treatment within the paradigm of a disease without a known cure, he was left with only managing the pathology. It is important to remember; however, that even the most targeted pharmaceutical treatment requires the body to act. As doctors, no matter what our interventions, we rely on the vital force to do the work of healing. What happens when we expand our understanding of cause to include the idea that illness can also be seen as a disturbance in the vital force, and that it can be the result of not only disease, but other assaults on the body that could potentially precede pathology?
Cause, Cure, and the Vital Force
As a naturopathic doctor, my intention and expectation with every patient is to help them cure their illness in the way that Hahnemann wrote about it in The Organon:
“The highest ideal of cure is rapid, gentle and permanent restoration of the health, or removal and annihilation of the disease in its whole extent, in the shortest, most reliable, and most harmless way, on easily comprehensible principles.”1
Dr Harold Dick, who was a student of Otis Carroll, who was a student of Henry Lindlahr, repeated the same process, more or less again and again, with each new patient. Rather than treat individual pathologies or diseases, Dr Dick treated the “ill person.” He was treating the vital force. His process was very similar each time: remove or moderate any known causes, stimulate the self-healing functions of the body, support the weakened or burdened systems or organs, correct physical structure as needed, and then get out of the way and let the vis medicatrix naturae bring about the restoration of health. Henry Lindlahr told us about the 3 primary causes of disease, which I have mentioned in my previous article. I will restate them, but in greater detail, along with the 3 secondary causes. It is important to note that though Lindlahr uses the term “disease,” he is not speaking about specific pathology. Similarly to Dr Dick recognizing and treating the “ill person,” Lindlahr is ultimately talking about cause and disease in terms of the vital force.
Causes of Disease (Adapted from Nature Cure, 1913)2
Primary:
- Lowered vitality due to overwork, nightwork, excesses, overstimulation, poisonous drugs, and ill- advised surgical operations.
- Abnormal composition of blood and lymph due to the improper selection and combination of food, poor digestion, and especially the lack of organic mineral salts and other essential nutritional elements.
- Accumulation of waste matter, morbid matter, and poisons due to the first two causes, as well as to faulty diet, overeating, the use of alcoholic and narcotic stimulants, drugs, vaccines, accidental poisoning, and to the suppression of acute diseases by poisonous drugs and surgical operations.
Secondary:
- Hereditary and constitutional taints of sycosis, scrofula, psora, syphilis; mercurianism, cinchonism, iodism (pharmaceutical effects), and many other forms of chronic poisoning.
- Fevers, inflammations, skin eruptions, chronic sinus discharges, ulcers, abscesses, germs, bacteria, parasites, etc.
- Mechanical subluxations, distortions, and displacements of bony structures, muscles, and ligaments.
Additionally, I would add to the list a 7th cause, the psycho/spiritual disturbances that accumulate in one’s life from the various traumas to which we are all subjected. Although I think Lindlahr did consider these kinds of things in Nature Cure, he did not refer to them specifically in the chapter where these other 6 are discussed. My experience has been that including the patient’s mental health history, their spirituality (in whatever form it may take), and any past traumas they have experienced, has proven invaluable when investigating cause.
How I Peel Back the Onion
In order to best understand cause, to understand why my patient is ill, and thereby, to know where to direct my efforts, I typically spend 1.5-2 hours with a new patient in a comprehensive evaluation. I begin by asking them why they have come and what it is that they want from me? This is essentially an exploration the chief complaint, though often there are several. I usually spend 15-20 minutes in initial discussion with the patient. I need to know the details. I take notes on a lined yellow legal pad, letter-sized, with a pen. I do not yet use an EMR, which are not legally required where I practice, and because I do not take insurance, I am not bound by insurance company requirements. Taking notes in this way allows me to focus on the patient, though with the right intention, I am sure that this can also be accomplished when typing information into a computer. During this time, patients will usually bring up any lab work they have had done (often they have brought copies with them). I will review it, and sometimes explain it to them. I will also make a copy for their file. I keep paper files. I have many thousands of these now, in steel file cabinets, filling two rooms in my clinic. This is one reason I may have to move to using an EMR.
Next I do what I call a “patho-biography,” in which I review the patient’s medical history. If they are older adults, I review their health in 5-year intervals. I ask questions like, “What was your health like from ages 5 through 10? Were there any illnesses or hospitalizations, etc.?” I always begin with the first year of life. I ask, “What was your health like as a baby? Did your mother say you were a healthy baby, you were colicky, or had some other health problem?” If they are under age 25, I will proceed in 3-year intervals. If they are under age 12, I will inquire 1 year at a time. I learn their health history in detail, the kinds of illnesses they have had, how they responded to them, and what kind of suppressions may have been employed.
After patients finish describing their health history, I complete a diet summary. I ask them, “What do you eat for breakfast, lunch, dinner, and snacks? Do you eat: eggs, meat, poultry, fish, cow’s milk, cheese, yogurt, butter, ice cream, fruit, salads, cooked vegetables, rice, potato, pasta, bread, sugar, or salt? Do you have any food reactions, cravings, or aversions?” I learn their eating habits and patterns, where they get their primary nutrients, and where there may be problems.
Next, I do a review of systems, from head to toe, to pick up on anything that may have been missed in reviewing their chief complaint(s). I also do a physical examination, the same Bates-type examinations we learned in school, with a number of additions that could be considered naturopathic, or functional considerations. These additions will depend on the chief complaint, but tend to include evaluation of pulse, tongue, iris, acoustic cardiogram, Bolen blood spot analysis, the Obermeyer test, and sometimes special tests such as Raglan’s test of adrenal function, calcium cuff testing, orthopedic exams, or spinal alignment.
I usually ask patients whether their childhood was safe, fun, happy? Some people tell me about their Tom Sawyer-like childhood, a delightful time. Others are silent for a moment, or start to cry, or look down at the floor and then reluctantly tell me about their abusive parents, or the divorce that wrecked their young life, or some other tragic experience that is still affecting their life and their health.
Then I ask them to tell me about their spiritual life. Some ask me what I mean by that. Some say they have none, or that they are a Catholic or a Muslim, or of some other religion. Some tell me they are spiritual, but not religious. Regardless, I get a sense of their internal (or external) support system, their world view, and explore how they see themselves in relationship to the larger universe.
Finally, I ask my patients whether I have missed anything of significance. All of this is takes me 90 minutes or more with a new patient, but I am looking for why they are ill, I am looking for what has disturbed their health. I am finding the cause, and it is time well spent.
The Acoustic Cardiogram
As mentioned, the acoustic cardiogram is one of the additional tests I use, and I find it helpful in directing my diagnosis and treatment. Dr. Dick used the acoustic cardiogram developed by Royal Lee in the 1920’s. While studying with him, I looked into getting one, but they cost several thousand dollars and I was barely out of school and with a young family. I didn’t have that kind of money. A friend of mine, a brilliant Czech naturopathic physician named Pavel Nyvlt, had developed a recording stethoscope, and I obtained one from him. It cost a couple of hundred dollars, which I could afford at the time. Pavel taught me the basic interpretation of the acoustic cardiogram, and I began to incorporate it into my practice. Since then, one of the American medical equipment companies has developed a recording stethoscope for teaching purposes. It has Bluetooth that connects it to my computer and costs around $400. I use it during every new patient visit to establish a baseline, and on most return patient visits to help track progress.
Sample Graphs
Since beginning with that first stethoscope from Pavel, I have recorded hundreds of acoustic cardiograms throughout my years in practice. They can tell you lots of useful information, and I have included 3 important sample graphs, which I also use for teaching purposes (See Graphs 1-3). For those interested in learning more about the technique, I would encourage you to reach out to one of the many practitioners or organizations that offer acoustic cardiogram training.
Graph 1
The first graph is the most perfect acoustic cardiogram I have ever recorded. It was recorded from a patient diagnosed with metastatic breast cancer, who came to me after having been told that she had less than a year to live. This particular graph was recorded 3 years after her initial diagnosis, 3 years after we started working together, and after her 300th constitutional hydrotherapy treatment. Note the flat baseline, the thin complexes, and the “tall-short, tall-short” pattern, in perfect rhythm.
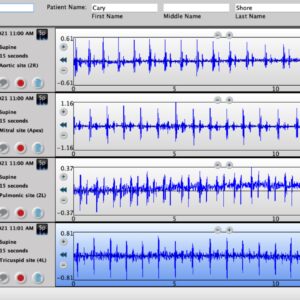
Graph 2
The second graph is recorded from a 14-year-old boy with adrenal fatigue. Note the typical “short-tall, short-tall” configuration in the first and third tracings, a sign of adrenal stress.

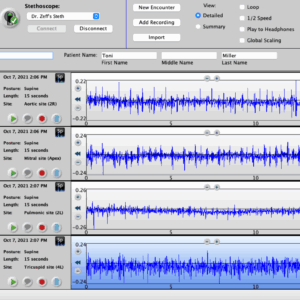
Graph 3
The third graph is a from a 20-year-old woman with asthma. Note the weakness (low amplitude) in the third tracing, which is over the pulmonary artery and lungs. The “fuzzy” baseline in the fourth tracing is the blood coming back to the heart from the intestine and liver, which is a visual demonstration of a toxic or inflammatory disturbance.
Not Quite “The End”
I had originally planned to complete only a 2-part series on the subject of “finding the cause”; however, I want to include some additional information about evaluation methods I find helpful. In my next article, I will discuss other diagnostic tools I use, add a few more pictures, and then tie it all together.
Respectfully,
Jared L. Zeff, ND, VNMI, Lac
References
- Hahnemann S. Samuel Hahnemann’s Organon of Homeopathic Medicine. 4th American ed. New York, NY: Radde; 1860.
- Lindlahr H. Nature Cure. Chicago, IL: Nature Cure Publishing Company; 1913.

Jared L. Zeff, ND, VNMI, LAc is a licensed doctor of naturopathic medicine and a licensed acupuncturist. In addition to functioning as Medical Director at the Salmon Creek Naturopathic Clinic in Vancouver, WA, Dr Zeff taught on the faculty at National University of Natural Medicine in Portland, OR, where he was also Dean from 1988 to 1993, and holds a professorship in Naturopathic Medicine. Dr Zeff is a graduate of the University of California, NCNM, and the Emperor’s College of Traditional Oriental Medicine. He, along with Pamela Snider, is the author of the AANP’s Definition of Naturopathic Medicine, and the Therapeutic Order concept.






{kind=link}