
By Steve Parcell, ND
According to the Sexual Function Health Council of the American Foundation for Urologic Disease, 30 million men in the United States are estimated to have some form of erectile dysfunction. Erectile dysfunction (ED) is defined as the inability to obtain or maintain penile erection sufficient for satisfactory sexual performance, lasting at least three months. The definition of erectile dysfunction distinguishes itself from other disorders such as inability to achieve orgasm, low libido, and premature ejaculation. ED has a significant impact on the quality of life and is a common problem. Its prevalence is directly proportional to aging and varies from 30% to 40% at age 40, to up to 70% at 70 years and older (Lue, 1995). One must comprehend the intricate mechanisms of erection in order to understand the underlying cause of dysfunction. Normal aging, as well as psychogenic, vascular, neurogenic, and endocrinologic causes, or those due to structural abnormalities of the penis, should be considered when attempting to determine its cause. Low libido has either a psychogenic or an endocrinologic component.
Erection is a complex, involuntary, neuropsychological, hormone-mediated vascular event. Alpha-adrenergically mediated contraction of cavernosal and vascular smooth muscle limits blood flow to the penis and maintains the usual flaccid state. An erection occurs when erotic stimuli, received via any of the five senses and processed in the hypothalamus, results in inhibition of sympathetic tone and release of nitric oxide (NO) from nonadrenergic, noncholinergic nerves and endothelial cells of the arterioles in the penis.
NO activates guanyl cyclase, thereby generating cyclic guanosine monophosphate (cGMP). cGMP decreases calcium uptake into vascular and cavernosal smooth muscle and induces relaxation. Smooth muscle relaxation permits engorgement of cavernosal sinusoids with blood and the development of an erection. In addition to NO, other neurotransmitters postulated to play a role in the erectile mechanism include prostaglandins, vasoactive intestinal peptide, serotonin, and dopamine (Cohan, 2001).
Ejaculation is reflex sympathetic discharge from the nerves of the penis to the seminal pathway, the muscle coats of the epididymis, ductus deferens, the seminal vesicles, and the prostate gland, causing the release of sperm and seminal fluid.
Any derangement in this sequence of neurovascular events can result in ED. For example, compromise of neural pathways either centrally (stroke) or peripherally (diabetic autonomic neuropathy) may lead to ED. Alternatively, venoocclusive failure may occur from intrapenile lesions (Peyronie’s disease) (Cohan, 2001).
Libido is the conscious feeling of the sexual urge, mediated by dopamine and sex hormones, which originates in the cerebral cortex. In the event of aroused libido, the brain center sends impulses to the spinal center, which in turn passes them to the nerves of the penis.
Recent findings suggest that ED has an organic cause 75% of the time. This finding contrasts with the previous view that more than three quarters of erectile dysfunction is of psychogenic origin. Organic causes include vascular disease, neurotransmitter imbalances, neurologic disease, hypogonadism, drug use, structural problems (e.g., Peyronie’s disease), and systemic diseases such as chronic renal failure and cancer.
Prescription drugs, narcotics, and alcohol are common causes and should always be ruled out first before referral to a urologist.
 Evaluation and treatment: (in chronological order)
Evaluation and treatment: (in chronological order)
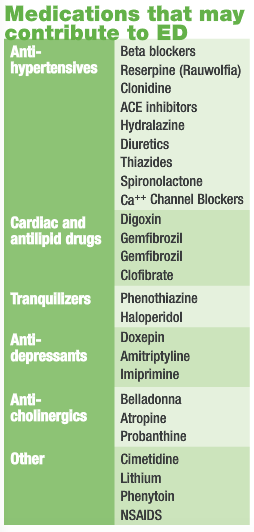
- First visit: Medical history and exam, ask patient why he thinks he has ED (stress, marital problems, etc.). This can often eliminate the need for further studies. Also rule out chronic systemic disease (renal failure) and neurological disease. Go through drug list (above). If possible, eliminate the need for drugs that cause ED.
- Endocrine causes: Serum free and total testosterone, FSH, LH, or salivary testosterone can determine if hypogonadism is present (Kirby, 1994). If total testosterone is low initiate androgen replacement therapy, checking PSA and testosterone levels every three months. If only free testosterone is low consider nettle and other agents that decrease testosterone binding to sex hormone binding globulin. Hypogonadism should be treated early, as a good response to androgen therapy is often seen.
- Psychogenic causes: Couples or individual counseling to help address anxiety, teach stress coping skills, and improve communication. Visualization and hypnotherapy may also be effective. Identifying the underlying issues is critical. If ED is nonorganic, yohimbe (Pausinystalia yohimbe) provides the best result (Vogt, 1997). I use 30 mg a day (two 5-mg tablets three times daily) for eight weeks. Side effects include palpitations and hypertension. Yohimbe does not work well for organic ED (Guay, 2002). Other botanical agents to consider are Panax ginseng and maca (Lepidium meyenii). Though less well known as a treatment for ED, we have been using maca with success recently. An effect of maca on sexual desire has been described in normal men treated with 1.5 or 3 g of maca per day during 12 weeks in a randomized double-blind trial (Córdova, 2001). In this study the effect of maca was compared with the effect of a placebo at 4, 8, and 12 weeks of treatment. An increase in sexual desire was noticeable in apparently healthy men taking maca at 8 and 12 weeks of treatment. Maca does not appear to affect serum sex hormone levels.
- Arginine: Arginine may help regardless of cause because it helps increase nitric oxide. I do a trial with 3 g for 3-4 weeks (Zorgniotti and Lizza, 1994).
- Second visit: If response is suboptimal to hormone therapy and botanicals and arginine, or testosterone is normal, do urine neurotransmitter testing (Neuroscience 888-342-7272). Neurotransmitter balances can cause or be caused by psychogenic factors. I do a urine assay and treat with targeted amino acid therapy (TAAT) as indicated. This may be done at initial visit as well.
- Third visit: If still no response, refer for sleep study or penile injections for diagnosis. This is important, because if there is a neurologic or vascular cause, agents like yohimbe, maca, and ginseng will not work well.
- Sleep study: Patients are monitored for rapid eye movement (REM) sleep, when an erection is seen. This rules out any organic cause (Karacan et al., 1977).
- Penile injections: When a small amount of alprostadil is injected into the penis it induces an erection in psychogenic ED, thus ruling out organic causes (Jordan, 1999).
- Duplex Doppler ultrasonography: This can be used to evaluate the arterial and venous blood flow of the penis and may provide details of pressure related to erectile dysfunction, which could be corrected with surgery (Jordan, 1999).
Summary: Although ED increases with age there is usually some reason why. Your patients may have been told that it’s “all part of aging” and that Viagra is their only option. They will appreciate a thorough workup as I have described. Patients on antidepressants respond well to the neurotransmitter therapy, maca, and yohimbe. Patients on cardiac drugs or antihypertensives should generally not be given yohimbe but may respond to maca, arginine, or TAAT. Patients wishing to discontinue tranquilizers and antidepressants must be tapered off slowly and supported with TAAT. Libido problems only (with no ED) respond well to testosterone and TAAT. If all else fails, try Viagra.
References
Cohan P: Erectile dysfunction, J Clin Endocrinol Metab 86(6):2391-4, 2001. Review.
Córdova A: Efecto del Lepidium meyenii (Maca) una planta alto-andina sobre el estado de ánimo y el deseo sexual en varones aparentemente normales, Reprodução e Climatério (Suppl)16:96–97, 2001.
Guay AT: Yohimbine treatment of organic erectile dysfunction in a dose-escalation trial,
Int J Impot Res 14(1):25-31, 2002.
Jordan GH: Erectile function and dysfunction, Post Graduate Med 105:62-72, 1999.
Karacan I et al: Nocturnal erections, differential diagnosis of impotence, and diabetes, Biol Psychiatry 12:373-80, 1977.
Kirby RS: Impotence: diagnosis and management of male erectile dysfunction, BMJ 308:957-61, 1994.
Lue TF: Male sexual dysfunction. In Tangho EA, McAnnich R (eds): Smith’s General Urology, ed 14, Norwalk, CT, 1995, Appleton, Lange, pp 772-92.
Vogt HJ: Double-blind, placebo-controlled safety and efficacy trial with yohimbine hydrochloride in the treatment of nonorganic erectile dysfunction, Int J Impot Res 9(3):155-61, 1997.
Zorgniotti AW, Lizza EF: Effect of large doses of the nitric oxide precursor, L-arginine, on erectile dysfunction, Int J Impot Res 6:33-6, 1994.
 Stephen W. Parcell, ND, is a licensed naturopathic physician and graduate of Bastyr University, with additional training at the American Academy for the Advancement of Medicine and the American Academy of Environmental Medicine. Dr. Parcell is certified in chelation therapy and, after completing the Autism Research Institute’s physician training program, a certified Defeat Autism Now (DAN) practitioner. He is past vice president of the Colorado Association of Naturopathic Physicians. Dr. Parcell currently works at NatureMed, LLC, a naturopathic medical clinic in Boulder. He can be reached at 303-884-7557.
Stephen W. Parcell, ND, is a licensed naturopathic physician and graduate of Bastyr University, with additional training at the American Academy for the Advancement of Medicine and the American Academy of Environmental Medicine. Dr. Parcell is certified in chelation therapy and, after completing the Autism Research Institute’s physician training program, a certified Defeat Autism Now (DAN) practitioner. He is past vice president of the Colorado Association of Naturopathic Physicians. Dr. Parcell currently works at NatureMed, LLC, a naturopathic medical clinic in Boulder. He can be reached at 303-884-7557.

















