
Tim Shannon, ND
March 2007
Patient is a seven-year-old boy … pleasant child, affable, charming, wearing a Spiderman shirt. Patient is sweet but reserved.
(Physician) Know why you’re here? No.
Things scared of? Swimming lessons. I don’t like holding my breath, I don’t like putting my head under water for a long time.
Something else that scares you? My brother. He rubs my hair, picks me up, pushes me really high on the swing, which I don’t like, or just that I don’t know what he’ll do.
Animals? I like alligators, dinosaurs, eagles. Favorite one? Probably alligators. I like how they bite people’s feet off, how they are in water and out of water at the same time, like turtles.
Sleep okay? I go to sleep at 8:30 p.m., I fall asleep around 11 p.m. I just lie in my bed, wait to go to sleep, think about different stuff.
Dream? I remember like 20. When I was six [years old], I dreamt I was at an amusement park, each kid was taking what they wanted. Then we were in the line to go home. We were on this bridge, one of my friends said we have to be still, but I didn’t listen. Then this monster jumped out of the water and bit my head off, but I could still see. I was about to fall into the creek, then I woke up.
You and your brother fight sometimes? Yeah.
Are you cautious or more of a risky type? I just like to jump out there even if I don’t know if it is safe.
Lots of friends? Yeah.
Do you prefer a certain temperature? I like to be colder more than warmer.
Music? It is my least favorite thing in school.
(Patient’s mother):
He is a bright fellow. He is here because he’s having a really hard time with his temper and is fairly rigid. He gets fixated on clothes, like a favorite sweatshirt, and will wear it for four or five weeks.
He was in the principal’s office for punching another kid in the eye and for punching a girl in the chest. He doesn’t follow limits very well, he’s reluctant to do what he’s told. He’s very short tempered.
He is very organized, makes his bed, gets upset if someone opens a closet door without closing it, if he doesn’t have control over things. He has a sacred space, it is very important for him. The violence, short temper and rigidity are issues. It’s been hyped up the last few weeks. He got stepped on by his brother by accident, and he was very dramatic about it. Early on in his life, he was a head banger. He is not commonly talkative. Does really well one on one, and has a hard time with groups.
More examples of anger, violence and destructiveness? In the morning, when we ask him to do simple things (like get up, get dressed, come upstairs), and he’ll yell “No!” or “I’m not ready!” Or he’ll ignore us, and after a third or fourth request, he’ll start yelling. When angry he can call us names. He says things to adults that are very strongly worded, like ‘shut up,’ or ‘you can’t make me.’ He even spit in my face once. He has a very strong sense of what is fair. If his brother has more ice cream then he has, he’ll throw an hour-long tantrum until he gets his way.
He is quick to hit, he’s bitten children, scratched and kicked. If there is some chaos, or people ganging up on him, he doesn’t cope very well. He hit his best friend, a girl that he adores, pretty hard because he was jealous of the other kids playing with her. She was hurt, crying and upset. For a long time he couldn’t show remorse, empathy or concern, he couldn’t make eye contact with her, or apologize.
Sympathy/Empathy? Not so empathetic. I experience him as a deeply passionate person, and caring, but not so expressive. If he’s responsible, if he’s injured someone, he is unable to make that shift. If his brother or an animal is injured, he’s there to help.
Clothing? He doesn’t like wearing tight clothes, gets very attached to clothing.
Jealousy? It translates into what he considers to be fair. If you do something for the other child, he assumes it will be done for him, too. When he was really little, he didn’t like a lot of touch.
Is he an audacious child (looking to confirm Rx)? Definitely. He’s working on his image to be a prankster, to mimic his older brother. He wants to one-up his older brother.
Competitive? Definitely. He loves charts and wants records, stars on how he’s done.
Ambitious? Yes.
Headaches? No.
Appetite? Fine, but limited to pizza and pasta.
Scared of? He’s been taking swimming lessons for several months; he’s afraid of drowning, he brings it up quite often.
Senses? He can be oversensitive with all of them. He has a particularly uncanny acuity of hearing. He can detect tiny sounds that no one else hears.
Baseline:
1) Violence/hitting: once per week
2) Obstinate: multiple times per day
3) Irritable/sullen with changes
4) Insistence to wear same clothing for weeks
5) Fear of drowning and swimming
Assessment & Comments
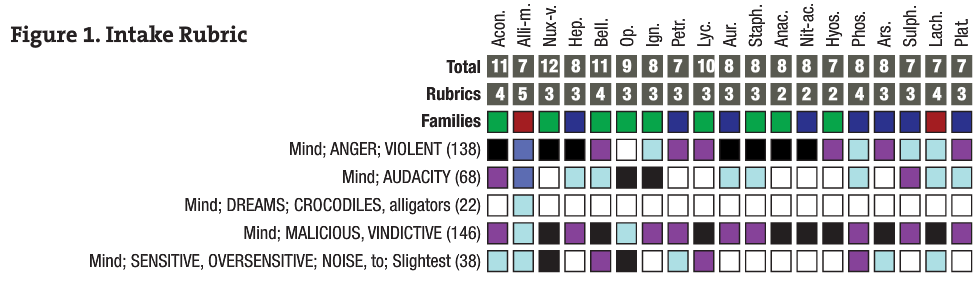
During the intake, I wondered if this could be a case of Alligator mississippiensis (Alli-m in Figure 1). The remedy had recently been proven by Dr. Todd Rowe. Over the years, I’ve noticed that some cases that require an animal remedy will either hate, fear or admire the animal they require. Of course, there needs to be more than a like or dislike of an animal to choose a remedy.
In this case, I saw there were some themes common to reptiles that I have seen before, such as: jealousy and competitiveness, audacity (audacity and disrespect for authority is more true for Lachesis, Bothrops and T-rex), averse to tight clothes, lacking empathy and a tendency to being more intellectual – a bit cold.
Another theme common to reptiles is an identification with the “dark” side. In this case, the patient’s interest in alligators was curious. He said he liked that they can bite people’s feet off. Also, the dream of a monster from the water biting off his head … He seemed quite pleased with himself while relating these images.
Another “soft” confirmatory was his fear of drowning. Again, sometimes patients who require certain animal medicines will have either an attraction or aversion to the environment where the animal lives. So I decided to trial him with a single dose of 30C, given in the office at the initial consult.
Besides the case fitting the above themes, I also repertorized the case. I had previously read about a cured case of this remedy. All this research supported my hypothesis that perhaps this child could require this new medicine.
Plan: Single dose of Alligator mississippiensis 30C
Case note: Two weeks later, the parents told me during their other son’s follow-up appointment that the boy had clearly improved, that there had been no aggravation and that his teachers had also commented on how much better his behavior had been.
April 2007
After the dose? (Mother): It immediately had an effect on the things we were looking at. He wasn’t hitting or using curse words as much. He even had more flexibility with clothing, and no significant negative behavioral encounters with the teacher or kids at school.
Overall there is a sense of him being more cooperative, but there are other power struggles. He used some strong language, especially after a weekend when he was with a lot of other children.
Compared to before the Rx? He was clearly better for a time after the dose, but he has regressed some. When he’s angry it is striking, almost frightening. His backtalk has an intense feeling behind it. It had abated after the Rx, so when it resurfaced it was noteworthy.
Baseline:
1) Violence/hitting: About half what it was.
2) Obstinate: Much better, once a day or every other day.
3) Irritable/sullen with changes: half as frequent.
4) Insistence to wear same clothing for weeks: He has some favorite clothes and gets really upset if they are not available.
5) Fear of drowning and swimming? (Patient): I’m not as scared, I just don’t like doing it.
Assessment and Plan: A good, but waning response. Repeat dry dose, 30C, split – one dose in a.m., one dose p.m.
June 2007
Feel different? (Patient): I’ve been acting different. In school I’ve not been punching as much. It is really good at home, I’ve not had one single fight with my brother.
Sleep? Good. I used to go to sleep at 11 p.m., now going to sleep at 9 p.m.
Anything else different? No.
How is he doing in general? (Mother): Markedly improved, just the last week slipped a bit. There is a sense of maturity, being clear about his own abilities. The issues about him being uncooperative, inflexible, short tempered – all those areas have improved. They still occur, but he is definitely more amenable, more spontaneous at helping at home. I think it has been enormously different.
Isolated? We noticed with friends and groups, he was always on the outside, had a hard time connecting with a dialog or interacting – more doing parallel play. Now he’s able to take turns, tell stories and listen; it’s more of a two-way street. It seems to have markedly improved and correlates with just after the last doses.
Baseline
1) Violence/hitting: Two or three incidents since last time. Something different about those episodes? It seems like they are a reaction to provocation, rather than him provoking.
2) Obstinate: Still some of that, mouthiness sometimes. That might happen three or four times a week now; it used to be more like several times per day.
4) Insistence to wear same clothing for week: Has not changed a whole lot.
5) Fear of drowning and swimming: (Patient): Now I’m not really nervous, I just don’t like the drills, but swimming is pretty fun.
Feel different about being in water? (Patient): Yeah. (Mother): That is definitely better.
Assessment and Plan: Good effect so far. Mother is concerned with the approaching summer because of his fragility around transitions. I gave him a single dry dose of 200C.
August 2007 Summary
Comments: The patient was doing well, but three weeks prior to this follow-up he began to regress. In this time he had an encounter with an older boy. The boy was asking him to do some inappropriate sexual things. It was unclear whether it was due to this incident that came out about this older boy or other stressors in the summer. But the patient began to lash out more and was beginning to have some difficulty falling asleep. Most of his baseline symptoms showed regression. Therefore, I suggested they repeat the 200C in a split dose – one dose in the a.m. and one in the p.m. of the same day.
Fall 2007 Case Note
There were multiple missed communications between the parents and me. During this time, the patient began to act out with violence, rudeness and oppositional behavior. It was hard to determine the cause, but it might have come from further contact with the boy in the neighborhood who was acting out sexually with the patient. Many attempts to coordinate a different type of dosing failed. Finally, I sent the parents a single dose of 200C in the beginning of October. The parents phoned me one month later that he was definitely improving again, though he seemed a bit apathetic. His mother was concerned about him due to his apathy. Just before Christmas he was beginning to show more rudeness and backtalk – though very little physical violence. I then gave a single dose of Alligator mississippiensis 1M.
February 2008
(Mother): He has trouble falling asleep, goes to bed at 8 p.m., still awake until 10 or 10:30 p.m. Had this difficulty with falling asleep since third grade. Otherwise, he’s doing well, more flexible. He’s been cooperative, more focused.
The 1M helped? Yes, it made a huge impact. It was two weeks after. It was given on December 16, and right after Christmas he began doing really well. With the short temper and obstinance he’s much better. At school he’s not great, though I think some of it has to do with school.
He’s much more flexible and open. He’s also more affectionate. The last few months there has been family stress. And he’s been really empathetic. He’s been very huggy, a wonderful thing for him.
The last 1M didn’t help with the sleep? No, it is several nights a week he’s struggling.
How often? Three or four nights a week. If he goes to sleep on his own, he tosses and turns. Can’t go to sleep without his brother in the bed.
Some change? There was the sexual stuff in summer with the neighbor, that had an impact.
Anger? He can still be belligerent, but now he’s reachable. There is also so much less of the angry expressions.
Assessment and Plan: Sounds like a good response. They may need to use the Rx for sleep difficulty, but may also be able to use melatonin. No doses for now, wait and watch.
May 2008
Wearing same clothes? (Patient): I like to wear the same clothes about three times a week. (Mother): He has his favorites, if asked he’ll change his clothes now. He will even wear dress-up clothes, that is big for him.
Mother (after patient has left room): The last dose worked great. He’s become a bit short tempered again, but not anywhere to where he was in the beginning. There were a few comments from his teacher, that he was not as well focused. Overall, he’s enormously improved, much more empathic, spontaneous … Partner and I have had some rough spots lately. She’s been more emotional, he’s been spontaneously going to hug her and try to take care of her. This empathy is really new for him – only after treatment began. He’s also asserting himself more with his brother, in a mature way.
They had an awesome interchange about one week ago. They were arguing, and he showed a wonderful ability to go from reactivity to being reasonable. Both of them have really changed on their respective remedies. But overall, he is showing less and less of the angry reactiveness. Overall he has his two feet on the ground more and more now. There is enormous change in him overall. He’s using his words much more, instead of violence.
Assessment: It sounds overall like a good response. Both parents are very happy with the results. All the baseline symptoms are either a great deal better or resolved. However, his sleep issues could use a bit more support, so I gave another 1M single dry dose. Given the overall good response, I told the mother that we are done with formal appointments.
 Tim Shannon, ND is in private practice in Portland. He specializes in the treatment of mental, emotional and behavioral health. He uses classical homeopathy to treat a wide range of mental health complaints: ADHD, OCD, PMS, autistic spectrum, depression, anxiety, eating disorders, PTSD, bi-polar, schizophrenia, etc. Dr. Shannon lectures at NCNM as well as to the local community on a variety of mental health complaints.
Tim Shannon, ND is in private practice in Portland. He specializes in the treatment of mental, emotional and behavioral health. He uses classical homeopathy to treat a wide range of mental health complaints: ADHD, OCD, PMS, autistic spectrum, depression, anxiety, eating disorders, PTSD, bi-polar, schizophrenia, etc. Dr. Shannon lectures at NCNM as well as to the local community on a variety of mental health complaints.

















