
Robert Kachko ND, LAc
Alzheimer’s disease (AD) has the historically unique distinction of being the only common chronic disease with no known prevention or cure. This proposition becomes increasingly ominous when considering the rising tide of Alzheimer’s expected to impact North America and the rest of the world in the next several decades. In the United States, 5.3 million people currently have AD (making up 75-80% of all dementia cases), and that number is expected to climb to a medically and economically unsustainable 13.8 million people by 2050.1
The idea that AD is recalcitrant to all interventions is grounded in a belief that has been largely disproven within the last decade – that the nervous system is static and categorically unchangeable. The large cost and consistency of failed drug trials over the last several decades leads us to 1 central conclusion: Alzheimer’s disease is a multifactorial phenomenon which develops over several decades prior to the onset of symptoms and is, in large part, a result of lifestyle.
Fortunately, the concept of neuroplasticity is quickly becoming mainstream. A 2014 study by UCLA, though small (improvement in 9 out of 10 participants), for the first time showed a reversal of mild to moderate AD using a comprehensive approach of individualized diet and lifestyle recommendations.2 Of all of the systemic factors at play, perhaps none is more crucial to address than insulin resistance.
“Diabetes of the Brain”
A key finding in our evolving understanding of relevant pathology is the strong correlation between AD and insulin resistance, metabolic syndrome, and type 2 diabetes (T2DM). In fact, as much as 40% of AD pathology has been attributed to hyperinsulinemia.3,4 Higher HbA1c levels correlate with lower cognitive capacity and changes in hippocampal microstructure, and positive APOE e4 genetic status (the most well-studied genetic determinant of AD risk) is correlated with increased risk of T2DM, altered lipid profiles, and cardiovascular disease.5,6 As long-standing impaired cerebral glucose metabolism is a central aspect of AD pathology, research suggests that intervention at midlife may be especially critical for outcome success.7 Further, successfully addressing diabetes in later life reduces the conversion of mild cognitive impairment to AD and all-cause dementia.8
Pathophysiology
It is also well known that the brain regions (especially the hippocampus) that rely most heavily on insulin and insulin-like growth factor (IGF) signaling are the most vulnerable to AD pathology.9,10 Impairments in brain insulin/IGF signaling lead to increased expression of amyloid-β precursor protein (AβPP) and accumulation of AβPP-Aβ aggregates.11 Some of the proposed mechanisms, all of which are at least partially amenable to naturopathic approaches, are listed in Figure 1.11
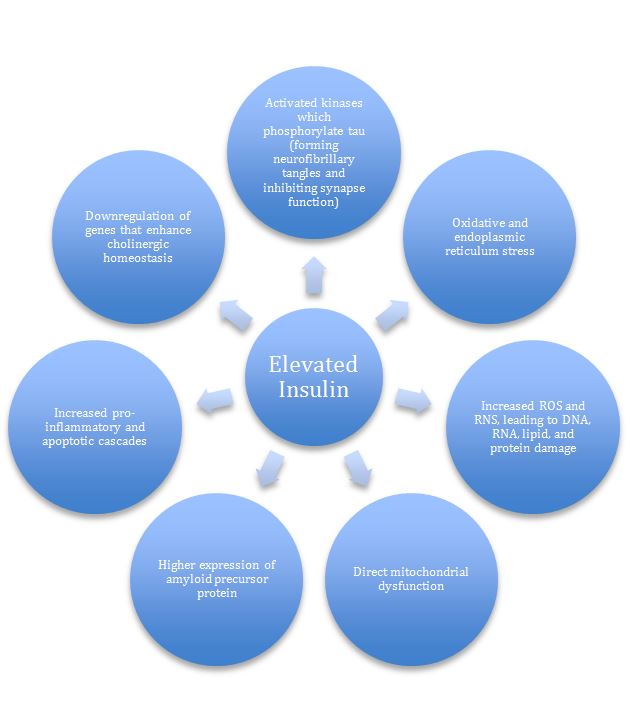
Figure 1. Hyperinsulinemia’s Effects on the Brain (Adapted from de la Monte SM, 2012)11
Three Dietary Approaches
A comprehensive approach to AD must be multifactorial (Table 2), but the foundation of any successful therapy for dementia must begin with diet. For AD, the foundation of a successful diet must account for blood sugar abnormalities. Strict sugar control is even more crucial in the elderly population, as taste preferences increase for calorie- and carbohydrate-rich, micronutrient-poor, sweet foods.12
MIND Your Diet
A hybrid Mediterranean and DASH diet (see Table 1), with several cognition-specific modifications, was studied in a population of 923 participants who were followed for 4.5 years. Aptly named the MIND diet, those who scored in the highest 1/3 of adherence (strict adherence) to the diet had a 53% risk reduction of developing AD.13 Just as impressive, those who were in the middle 1/3 (moderate adherence) had a 35% risk reduction.
For the majority of patients consulting a naturopathic physician, though, adherence to this diet will not seem especially strict; for example, a positive score was obtained by limiting red meat to a still-excessive 4 times per week. Also, the glycemic index of foods consumed was not a considered measurable, providing a further opportunity to optimize the diet. Even still, the MIND diet was associated with a slower rate of cognitive decline equivalent to 7.5 years of mental age. While the study outcome relates more to prevention than treatment, the same principles can be applied to individuals with an early diagnosis, as pathological changes typically occur long before symptoms set in.
Table 1. MIND Diet Used in Clinical Study13
| Foods to Eat
· Green leafy vegetables (eg, spinach and salad greens): At least 6 servings/wk · Other vegetables: At least 1 serving/day · Nuts: 5 servings/wk · Berries: 2 or more servings/wk · Beans: At least 3 servings/wk · Whole grains: 3 or more servings/day · Fish: Once per week · Poultry (eg, chicken or turkey): 2 times/wk · Olive oil: Use it as your main cooking oil · Wine: 1 glass/day |
| Foods to Avoid
· Red meat: Fewer than 4 servings/wk · Butter & margarine: Less than 1 tbsp/day · Cheese: Less than 1 serving/wk · Pastries & sweets: Fewer than 5 servings/wk · Fried or fast food: Less than 1 serving/wk |
Therapeutic Fasting
Therapeutic fasting has long been an approach of the hygienic physicians, and it was relied upon heavily in the origins of nature cure. In industrialized countries where (fast) food is readily available, the population is overeating at unprecedented rates. A higher intake of calories and fat in 980 elderly individuals studied over 4 years was associated with 2.3-fold higher AD risk, but only in those who were APOE4+.14 In an 18-year study, those who habitually consumed fewer calories had lower AD rates, and for every 1.0 increase in BMI at age 70, AD risk increased by 36%.15 In a review of the metabolic effects of calorie-restricted or intermittent-fasting diets, insulin sensitivity measured via HOMA-IR correlated well with weight loss in most studies; 1 typical study correlated an 8% weight loss to a 33% improvement in insulin sensitivity. Similarly, reductions in fasting insulin of 20-31% were noted after 8-12 weeks of treatment.16 In most studies of intermittent or alternate-day fasting, visceral fat loss parallels overall weight loss, on the order of 4-7% over 6-24 weeks of treatment.16
While sufficient long-term outcome studies in humans are currently lacking (many animal studies have been conducted), several small trials exist. Caloric restriction (CR) of 3-4 months improved cognitive function in the elderly, as measured by verbal memory scores, in parallel with reduced fasting insulin and C-reactive protein (CRP).17
There are several potential cellular mechanisms involved with these diets (thought mostly to result from the hormetic effect of energy restriction), the best studied of which include reduced oxidative stress, improved cellular bioenergetics, enhanced neurotrophic factor signaling (BDNF and FGF2), and reduced inflammation (reduced TNFα, IL-1β and IL-6).18,19 While many variations of caloric restriction and intermittent fasting exist, higher compliance and safety profiles are expected with daily overnight fasts (ranging from a minimum of 12 hours to 16 or 18 hours) compared to longer fasts. Of course, every patient should be assessed on an individual basis and carefully monitored throughout treatment.
Ketogenic Diets
Another key benefit of intermittent fasting or caloric restriction is the induction of ketosis after 12-16 hours of fasting. Glucose hypometabolism (leading to chronic brain energy deprivation) in AD patients is roughly 20-25% lower than in age-matched, cognitively-normal individuals.20 In those prone to diabetes, these changes are often most pronounced in the frontal cortex, and in some can be discovered at ages as young as 24 years old.21 Importantly, the ability to produce and utilize ketone bodies as an alternate substrate may actually increase with age and with insulin resistance (which causes an increase in monocarboxylate transporters).22,23 While we only have 33 g/day of glucose from glycogen stores, the average human brain metabolizes 110-145 g/day of glucose for ATP production. For this reason, an alternate fuel source is required and fortunately provided by nature: ketone bodies (specifically beta-hydroxybutyrate and acetoacetate, which are beta-oxidized in the liver from long-chain fatty acids).
Ketogenic diets tend to be high in fat and restrictive of carbohydrates. A common macronutrient profile would include a maximum 30 g carbohydrate, 1 g protein/kg body weight, and the rest of calories from fat (20% saturated / 80% polyunsaturated and monounsaturated). An alternative that is likely to meet with higher compliance is the direct consumption of medium-chain triglycerides (MCTs), most readily available in coconut oil, which increase ketone body levels regardless of macronutrient intake; MCT oils provide a linear dose-response relationship to increased plasma ketones. A therapeutic dose is 2 tbsp of organic virgin coconut oil per day, which provides on average 20 g of MCTs.24 This dose should be titrated gradually to avoid digestive disturbance. Otherwise, MCT oils have been shown to be safe, with a 30-day treatment of 30 g/day of MCTs not adversely affecting body weight, body fat content, body mass index, serum glucose, insulin, triglycerides, cholesterol, or free fatty acids.25
Conclusion
True familial Alzheimer’s disease is exceedingly rare, and while there is a genetic component (positive APOE4 status), this effect can be mitigated with a naturopathic approach. AD is, of course, a disease manifesting in end-organ brain pathology. Viewed in this reductionist way, it is likely to continue to be a burden plaguing the industrialized world in increasing numbers. However, if approached as a systemic disease with brain-specific susceptibility, perhaps the naturopathic profession can be at the forefront of preserving all which is at stake.
Table 2. A Multifactorial Approach to Alzheimer’s Disease
| Intervention | Study Outcomes |
| Vitamin E | 2000 IU/d alpha-tocopherol delayed clinical progression of 19% per year compared with placebo in mild to moderate AD26 |
| Vitamin D | Compared to those with 25OHD levels >50 nmol/L…
Severe deficiency (<25 nmol/L) was associated with a 122% increased risk of all-cause dementia; and deficiency (25-50 nmol/L) was associated with a 51% increased risk27 |
| Docosahexaenoic acid (DHA) | Epidemiological28 and intervention29 studies show improvements in memory |
| B Vitamins / Homocysteine-lowering | Treatment with B complex in subjects with homocysteine >11.3 µmol/L led to improvements in global cognition (MMSE), episodic memory, and semantic memory30
Brain atrophy (& homocysteine >13 µmol/L) was 53% less in the active B-vitamin treatment group31 |
| Meditation | Mindfulness-based stress reduction for 8 wks led to increased functional connectivity and reduced hippocampal atrophy32 |
| Social engagement | Remaining or becoming socially/physically active over a 10-year period was associated with up to a 49% decrease in dementia risk over the subsequent 10 years33
Quality of relationships appears more important than quantity34 |
| Cognitive engagement | History of lifelong cognitive activity may support better cognitive performance; this relation is mediated by a mechanism independent of Aβ burden35 |
| Aerobic exercise | A 2016 meta-analysis showed improvements in dementia specifically with aerobic but not other exercise36 |
| Environmental toxicity | Neurotoxic metals such as lead, mercury, aluminum, cadmium, and arsenic, as well as some pesticides and metal-based nanoparticles, have been involved in AD due to their ability to increase Aβ peptide and the phosphorylation of P-Tau37 |
| Acupuncture | A meta-analysis found a statistically significant difference between acupuncture plus donepezil vs donepezil alone in improving the MMSE score38 |
| Sleep | Melatonin (0.5 mg) in mild to moderate AD was linked to improvement in sleep parameters and MMSE scores (1.5 points) after 24 weeks, whereas the placebo group MMSE scores deteriorated by 2.8 points39 |
(25OHD = 25-hydroxyvitamin D; Aβ = beta-amyloid; P-Tau = tau protein; MMSE = Mini-Mental State Exam)
 Robert Kachko ND, LAc, sees patients at Inner Source Health-Manhattan, with a practice focus in healthy aging, and neurodegenerative and cardiovascular disease. He proudly serves on the Board of Directors and as Chair of the Public Education and Media Affairs Committee of the AANP, and on the legislative committee of the NY Association of Naturopathic Physicians (NYANP). He also serves as a clinical research consultant for Weill Cornell Medical’s Alzheimer’s Prevention Clinic and on the Medical and Dental Advisory Board for Sharp Again Naturally, a non-profit committed to addressing healthy aging, as well as Alzheimer’s/Dementia care from a natural perspective.
Robert Kachko ND, LAc, sees patients at Inner Source Health-Manhattan, with a practice focus in healthy aging, and neurodegenerative and cardiovascular disease. He proudly serves on the Board of Directors and as Chair of the Public Education and Media Affairs Committee of the AANP, and on the legislative committee of the NY Association of Naturopathic Physicians (NYANP). He also serves as a clinical research consultant for Weill Cornell Medical’s Alzheimer’s Prevention Clinic and on the Medical and Dental Advisory Board for Sharp Again Naturally, a non-profit committed to addressing healthy aging, as well as Alzheimer’s/Dementia care from a natural perspective.
References
- Alzheimer’s Association. Alzheimer’s disease facts and figures. Alzheimers Dement. 2015;11(3):332-384.
- Bredesen DE. Reversal of cognitive decline: a novel therapeutic program. Aging (Albany NY). 2014;6(9):707-717.
- Biessels GJ, Staekenborg S, Brunner E, et al. Risk of dementia in diabetes mellitus: a systematic review. Lancet Neurol. 2006;5(1):64-74.
- Kopf D, Frolich L. Risk of incident Alzheimer’s disease in diabetic patients: a systematic review of prospective trials. J Alzheimers Dis. 2009;16(4):677-685.
- Kerti L, Witte AV, Winkler A, et al. Higher glucose levels associated with lower memory and reduced hippocampal microstructure. 2013;81(20):1746-1752.
- El-Lebedy D, Raslan HM, Mohammed AM. Apolipoprotein E gene polymorphism and risk of type 2 diabetes and cardiovascular disease. Cardiovasc Diabetol. 2016;15:12.
- Willette AA, Bendlin BB, Starks EJ, et al. Association of Insulin Resistance With Cerebral Glucose Uptake in Late Middle-Aged Adults at Risk for Alzheimer Disease. JAMA Neurol. 2015;72(9):1013-1020.
- Cooper CC, Sommerlad A, Lyketsos CG, Livingston G. Modifiable predictors of dementia in mild cognitive impairment: a systematic review and meta-analysis. Am J Psychiatry. 2015;172(4):323-334.
- de la Monte SM, Wands JR. Review of insulin and insulin-like growth factor expression, signaling, and malfunction in the central nervous system: relevance to Alzheimer’s disease. J Alzheimers Dis. 2005;7(1):45-61.
- Freude S, Schilbach K, Schubert M. The role of IGF-1 receptor and insulin receptor signaling for the pathogenesis of Alzheimer’s disease: from model organisms to human disease. Curr Alzheimer Res. 2009;6(3):213-223.
- de la Monte SM. Contributions of Brain Insulin Resistance and Deficiency in Amyloid-Related Neurodegeneration in Alzheimer’s Disease. Drugs. 2012;72(1):49-66.
- Mundas D, Cooper JK, Weiler PG, et al. Dietary preference for sweet foods for patients with dementia. J Am Geriatr Soc. 1990;38(9):999-1007.
- Morris MM, Tangney CC, Wang Y, et al. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement. 2015;11(9):1007-1014.
- Luchsinger JA, Tang MX, Shea S, Mayeux R. Caloric intake and the risk of Alzheimer disease. Arch Neurol. 2002;59(8):1258-1263.
- Gustafson D, Rothenberg E, Blennow K, et al. An 18-year follow-up of overweight and risk of Alzheimer disease. Arch Intern Med. 2003;163(13):1524-1528.
- Barnosky AR, Hoddy KK, Unterman TG, Varady KA. Intermittent fasting vs daily calorie restriction for type 2 diabetes prevention: a review of human findings. Transl Res. 2014;164(4):302-311.
- Witte AV, Fobker M, Gellner R, et al. Caloric restriction improves memory in elderly Proc Natl Acad Sci U S A. 2009;106(4):1255-1260.
- Mattson MP. Energy intake and exercise as determinants of brain health and vulnerability to injury and disease. Cell Metab. 2012;16(6):706-722.
- Arumugam TV, Phillips TM, Cheng A, et al. Age and energy intake interact to modify cell stress pathways and stroke outcome. Ann Neurol. 2010;67(1):41-52.
- Cunnane S, Nugent S, Roy M, et al. Brain fuel metabolism, aging, and Alzheimer’s disease. 2011;27(1):3-20.
- Castellano CA, Baillargeon JP, Nugent S, et al. Regional brain glucose hypometabolism in young women with polycystic ovary syndrome: possible link to mild insulin resistance. PLoS One. 2015;10(12):e0144116.
- London ED, Margolin RA, Duara R, et al. Effects of fasting on ketone body concentrations in healthy men of different ages. J Gerontol. 1986;41(5):599-604.
- Robinson AM, Williamson DH. Physiological roles of ketone bodies as substrates and signals in mammalian tissues. Physiol Rev. 1980;60(1):143-187.
- Cunnane SC, Courchesne-Loyer A, St-Pierre V, et al. Can ketones compensate for deteriorating brain glucose uptake during aging? Implications for the risk and treatment of Alzheimer’s disease. Ann N Y Acad Sci. 2016;1367(1):12-20.
- Courchesne-Loyer A, Fortier M, Tremblay-Mercier J, et al. Stimulation of mild, sustained ketonemia by medium-chain triacylglycerols in healthy humans: estimated potential contribution to brain energy metabolism. Nutrition. 2013;29(4):635-640.
- Dysken MW, Sano M, Asthana S, et al. Effect of vitamin E and memantine on functional decline in Alzheimer disease: the TEAM-AD VA cooperative randomized trial. JAMA. 2014;311(1):33-44.
- Littlejohns TJ, Henley WE, Lang IA, et al. Vitamin D and the risk of dementia and Alzheimer disease. Neurology. 2014;83(10):920-928.
- Yurko-Mauro K, Alexander DD, Van Elswyk ME. Docosahexaenoic acid and adult memory: a systematic review and meta-analysis. PLoS One. 2015;10(3):e0120391.
- Yurko-Mauro K, McCarthy D, Rom D, et al. Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline. Alzheimers Dement. 2010;6(6):456-464.
- de Jager CA, Oulhaj A, Jacoby R, et al. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: a randomized controlled trial. Int J Geriatr Psychiatry. 2012;27(6):592-600.
- Smith AD, Smith SM, de Jager CA, et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One. 2010;5(9):e12244.
- Wells RE, Yeh GY, Kerr CE, et al. Meditation’s impact on default mode network & hippocampus in mild cognitive impairment: a pilot study. Neurosci Lett. 2013;556:15-19.
- Foubert-Samier A, Le Goff M, Helmer C, et al. Change in leisure and social activities and risk of dementia in elderly cohort. J Nutr Health Aging. 2014;18(10):876-882.
- Amieva H, Stoykova R, Matharan F, et al. What aspects of social network are protective for dementia? Not the quantity but the quality of social interactions is protective up to 15 years later. Psychosom Med. 2010;72(9):905-911.
- Gidicsin CM, Maye JE, Locascio JJ, et al. Cognitive activity relates to cognitive performance but not to Alzheimer disease biomarkers. Neurology. 2015;85(1):48-55.
- Groot C, Hooghiemstra AM, Raijmakers PJ, et al. The effect of physical activity on cognitive function in patients with dementia: A meta-analysis of randomized control trials. Ageing Res Rev. 2016;25:13-23.
- Chin-Chan M, Navarro-Yepes J, Quintanilla-Vega B. Environmental pollutants as risk factors for neurodegenerative disorders: Alzheimer and Parkinson diseases. Front Cell Neurosci. 2015;9:124.
- Zhou J, Peng W, Xu M, et al. The effectiveness and safety of acupuncture for patients with Alzheimer disease: a systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore). 2015;94(22):e933.
- Wade AG, Farmer M, Harari G, et al. Add‐on prolonged‐release melatonin for cognitive function and sleep in mild to moderate Alzheimer’s disease: a 6‐month, randomized, placebo controlled, multicenter trial. Clin Interv Aging. 2014;9:947-

















