

Proton Pump Inhibitors: For Better or Worse?
Steven Sandberg-Lewis, ND
Proton pump inhibitors (PPIs) are a $13 billion a year industry in the U.S. There were 95 million prescriptions written for these in 2005. Omeprazole, the first PPI to be synthesized, is also available over the counter. These drugs are indicated for the treatment of gastroesophageal reflux disease (GERD), Barrett’s esophagus and peptic ulcer disease, and to aid in the eradication of H. pylori overgrowth.
Effects on Gastric Secretion
PPIs block the H+/K+ ATPase enzyme system on parietal cells. This action increases pepsinogen and gastrin, and lowers pepsin and HCl. This increases gastric nitrate-rendering bacteria levels and increases carcinogenic nitrosamines in gastric juice. A resting pH >4 in gastric juices allows the possibility of bacterial overgrowth. In one study, 37% of patients on omeprazole had overgrowth compared to 10% of those in the control group (Theisen et al., 2000).
Hypergastrinemia has seve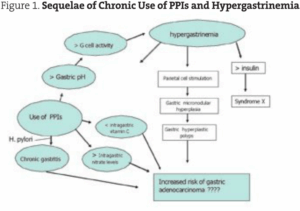 ral implications that increase the risk of gastric polyps and may have relevance to gastric and colon cancer. “In the long term, hypergastrinemia [induced by PPIs] causes enterochromaffin-like (ECL) cell hyperplasia and carcinoids” (Waldum, 2002).
ral implications that increase the risk of gastric polyps and may have relevance to gastric and colon cancer. “In the long term, hypergastrinemia [induced by PPIs] causes enterochromaffin-like (ECL) cell hyperplasia and carcinoids” (Waldum, 2002).
According to one retrospective analysis, gastric hyperplastic polyps are usually multiple, <1cm and sessile, and occur after a mean of 32.5 months on PPIs. Most carcinoids develop in patients with long-lasting hypergastrinemia and are of ECL origin. It is estimated that in humans it takes at least ten years to induce ECL cell carcinoids (Choudhry, 1998).
Hypergastrinemia also decreases intragastric vitamin C levels and may increase serum insulin (Jang, 2003; see Figure 1).
Effects on Duodenogastric Reflux (Bile Reflux)
In a study of 23 esophagitis patients on PPIs, acid and bile reflux decreased in most patients, but increased in 12% (Menges, 2001). Another study revealed abnormal bile reflux persisted in 48% of patients with Barrett’s esophagus receiving PPI therapy. Only 35% of the subjects’ acid reflux and bile reflux were normalized by the treatment (Sarela, 2004).
Effect on Gastric and Colonic Adenocarcinoma
Research suggests that gastrinoma (carcinoid tumor) diagnosis is delayed by PPI suppression of symptoms. More advanced disease is seen, and the five-year survival rate decreases in these cases.
“Physicians must maintain a high index of suspicion for this disease and not mask a potential malignancy with prolonged control of acid-related symptoms without taking steps to diagnose gastrinoma” (Ellison and Sparks, 2003).
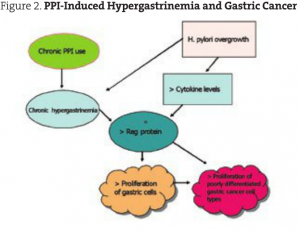 Reg protein is expressed in gastric fundic ECL cells. It is stimulated by gastrin, H. pylori overgrowth and certain cytokines (CINC-2 beta). Its effect is to increase proliferation of gastric mucosal cells. Reg protein is produced in many gastric cancer cells, especially the more advanced and poorly differentiated types. The hypergastrinemia induced by PPIs may increase this proliferation of gastric cancer cells (Kinoshita, 2004). On a similar note, a British study investigated the effect of PPI-induced hypergastrinemia on human colonic adenoma. They found that the use of omeprazole and lansoprazole increased the weight of human adenomas by 43%-70% (Watson, 2002; see Figure 2).
Reg protein is expressed in gastric fundic ECL cells. It is stimulated by gastrin, H. pylori overgrowth and certain cytokines (CINC-2 beta). Its effect is to increase proliferation of gastric mucosal cells. Reg protein is produced in many gastric cancer cells, especially the more advanced and poorly differentiated types. The hypergastrinemia induced by PPIs may increase this proliferation of gastric cancer cells (Kinoshita, 2004). On a similar note, a British study investigated the effect of PPI-induced hypergastrinemia on human colonic adenoma. They found that the use of omeprazole and lansoprazole increased the weight of human adenomas by 43%-70% (Watson, 2002; see Figure 2).
 Effect on Osseous Health
Effect on Osseous Health
Of no surprise to NDs is an increased risk of hip fracture in women older than age 50 on long-term acid suppression therapy. When these women take PPIs for greater than a year, they have a 44% increased risk of hip fractures. In addition, long-term, high-dose use increases hip fracture by 245% (Yang et al., 2006). No increase in fracture risk was found for H2 receptor antagonists.
“In vitro calcium carbonate disintegration and dissolution is pH dependent; as pH increases, disintegration and dissolution slows, decreasing from 96% at a pH of 1.0 to 23% at a pH of 6.1. Proton pump inhibitors effectively reduce gastric acid production and increase gastric pH to an average of 5.5, with 19% of the day spent above a pH of 6.0.”
Compared to placebo, omeprazole decreased calcium absorption by 41% in a seven-day trial (O’Connell, 2005).
 Effect on the Risk for Pneumonia
Effect on the Risk for Pneumonia
Use of gastric suppressive therapy is associated with a 1.89 relative risk for community-acquired pneumonia, while H2 receptor antagonists have shown a 1.63-fold increased risk (Laheij, 2004). The author theorizes that the increased risk was probably due to an increase in aspiration of gastric secretions in patients whose reflux was rendered less symptomatic by PPIs.
Clearly, the naturopathic approach to digestive wellness with a focus on improving function is an ideal approach. Optimizing the tone of the lower esophageal sphincter and the parasympathetic nervous system, and normalizing gastric and pancreatic secretion with resultant normalization of reflux symptoms, is a sane response to GERD. I agree with the following quote from the Digestive and Liver Disease journal: “The relatively common use of acid inhibitors in uncomplicated GERD or in the prevention of NSAID and steroid gastropathy is often unsubstantiated and should be limited to very specific situations.”
Amen.
 Steven Sandberg-Lewis, ND, DHANP, has been a practicing naturopathic physician since his graduation from National University of Natural Medicine (NUNM) in 1978. He has been a professor at NUNM since 1985, teaching a variety of courses but primarily focusing on gastroenterology and GI physical medicine. His clinic rotations are particularly popular among NUNM doctoral students. In addition to supervising clinical rotations he also maintains a part-time practice at 8Hearts Health and Wellness in Portland, Oregon.
Steven Sandberg-Lewis, ND, DHANP, has been a practicing naturopathic physician since his graduation from National University of Natural Medicine (NUNM) in 1978. He has been a professor at NUNM since 1985, teaching a variety of courses but primarily focusing on gastroenterology and GI physical medicine. His clinic rotations are particularly popular among NUNM doctoral students. In addition to supervising clinical rotations he also maintains a part-time practice at 8Hearts Health and Wellness in Portland, Oregon.
He is a popular international lecturer at functional medicine seminars, presents webinars, writes articles for NDNR and the Townsend Letter and is frequently interviewed on issues of digestive health and disease. He is the author of the medical textbook Functional Gastroenterology: Assessing and Addressing the Causes of Functional Digestive Disorders, Second Edition, 2017, which is available at amazon.com. In 2010 he co-founded the SIBO Center at NUNM which is one of only four centers in the USA for Small Intestine Bacterial Overgrowth diagnosis, treatment, education and research. In 2014 he was named one of the “Top Docs” in Portland monthly magazine’s yearly healthcare issue and in 2015 was inducted into the OANP/NUNM Hall of Fame.
Within gastroenterology, he has special interest and expertise in inflammatory bowel disease (including microscopic colitis), irritable bowel syndrome (including post-infectious IBS), Small Intestine Bacterial Overgrowth (SIBO), hiatal hernia, gastroesophageal and bile reflux (GERD), biliary dyskinesia, and chronic states of nausea and vomiting.
Many of the patients referred to Dr. Sandberg-Lewis have digestive conditions that have defied diagnosis and effective resolution. Often these patients desire naturopathic treatment options in lieu of the courses of treatments they have previously undergone. He understands diseases of the gastrointestinal tract, but also can assess function and often find successful treatments to regain a balance in the digestive system.
Dr. Sandberg-Lewis lives in Portland with his wife, Kayle. His interests include mandolin, guitar and voice; cross country skiing; writing and lecturing.
References
Theisen J et al: Suppression of gastric acid secretion in patients with gastroesophageal reflux disease results in gastric bacterial overgrowth and deconjugation of bile acids, J Gastrointest Surg 4(1):50-54, 2000.
Waldum HL et al: Long-term safety of proton pump inhibitors: risks of gastric neoplasia and infections, Expert Opin Drug Saf 1(1):29-38, 2002.
Choudhry U et al: Proton pump inhibitor-associated gastric polyps: a retrospective analysis of their frequency, and endoscopic, histologic, and ultrastructural characteristics, Am J Clin Pathol 110(5):615-21, 1998.
Jang JY et al: Randomized prospective trial of the effect of induced hypergastrinemia on the prevention of pancreatic atrophy after pancreatoduodenectomy in humans, Ann Surg 237(4):522-9, 2003.
Kato S et al: Mechanism of gastric hyperemic response during acid secretion in rats, J Clin Gastroenterol 25 Suppl 1:S48-55, 1997.
Menges M et al: Increased acid and bile reflux in Barrett’s esophagus compared to reflux esophagitis, and effect of proton pump inhibitor therapy, Am J Gastroenterol 96(2):331-337, 2001.
Sarela AI et al: Persistent acid and bile reflux in asymptomatic patients with Barrett esophagus receiving proton pump inhibitor therapy, Arch Surg 139(5):547-51, 2004.
Ellison EC, Sparks J: Zollinger-Ellison syndrome in the era of effective acid suppression: are we unknowingly growing tumors?, Am J Surg 186(3):245-8, 2003.
Kinoshita Y et al: Reg protein is a unique growth factor of gastric mucosal cells, J Gastroenterol 39(6):507-13, 2004.
Watson SA et al: Potential role of endocrine gastrin in the colonic adenoma carcinoma sequence, Br J Cancer 87(5):567-73, 2002.
Geller JL, Adams JS: Proton pump inhibitor therapy and hip fracture risk, JAMA 297(13):1429, 2007.
O’Connell MB et al: Effects of proton pump inhibitors on calcium carbonate absorption in women: a randomized crossover trial, Am J Med 118(7):778-81, 2005.
Laheij RJF et al: Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs, JAMA 292:1955-1960, 2004.
Horn J: Review article: relationship between the metabolism and efficacy of proton pump inhibitors–focus on rabeprazole, Aliment Pharmacol Ther 20 Suppl 6:11-9, 2004.
Marchetti F et al: Proton pump inhibitors in children: a review, Dig Liver Dis 35(10):738-46, 2003.
Hagiwara et al: Development of pancreatic acinar cell metaplasia after successful administration of omeprazole for 6 months in rats, Dig Dis Sci 52(5):1219-24, 2007.
Schillinger W et al: Negative inotropy of the gastric proton pump inhibitor pantoprazole in myocardium from humans and rabbits:evaluation of mechanisms, Circulation 116(1):57-66, 2007.
Yang et al: Long-term proton pump inhibitor therapy and risk of hip fracture, JAMA 296:2947-53, 2006.







{kind=link}