
Teerawong Kasiolarn, ND, MSAc, LAc
Tolle Totum
This article is a continuation of the case I presented in last month’s issue of NDNR. Part 1 provided an overview of metabolic syndrome (MetSyn) and its relationship with heart disease, an introduction of the naturopathic case study (see below), and a detailed discussion of the patient’s cardiometabolic laboratory workup and results.
As mentioned in Part 1, MetSyn is a strong risk factor for developing heart disease. Fortunately, naturopathic medicine represents a powerful therapeutic option for helping to prevent and reverse MetSyn. In this article, I outline the patient’s comprehensive naturopathic treatment plan, as well as his final lab results following 6 months of treatment.
Brief Review of Case
A 36-year-old Asian male came to see me for an initial naturopathic consult, with the chief complaint of fatigue for a few years. The patient’s weight had also been steadily increasing over the previous 5 years due to physical inactivity and poor eating habits. He is married, has 2 young children, and is self-employed. He had been working long hours with moderate stress for several years. However, he reported sleeping well.
The patient wanted to understand the underlying causes of his fatigue besides working too much. He has a strong family history of diabetes and heart disease, and wished to prevent any future cardiac events if possible. His ultimate goals were to feel well again with good energy, to lose weight, and to optimize his health.
The patient reported having no chronic health issues, took no prescription medications, and only used an OTC antihistamine as needed for seasonal allergies. He denied any alcohol intake or cigarette smoking. He took no nutritional supplements but was interested to hear our recommendations.
Since naturopathic doctors are not licensed in VA, I referred this patient one of our medical providers in the same medical group for an annual physical exam along with my recommended comprehensive laboratory assessment. His physical exam revealed that he was 170.18 cm (67 in) tall and weighed 104.3 kg (239 lb; BMI 36.0 kg/m2). His overall physical examination was unremarkable except having a Class II Obesity with significant central obesity (waist circumference 36.5 in).
Initial Laboratory Results
Here is a summary of the patient’s initial comprehensive lab results:
- Complete Blood Count (CBC) & Comprehensive Thyroid Panel (TSH, free T3, total T3, free T4, total T4, Reverse T3, anti-TPO & anti-Thyroglobulin antibodies): All normal results
- Comprehensive Metabolic Panel (CMP): All within normal limits except for borderline-high Fasting Glucose (94 mg/dL) and ALT (40 U/L) levels, and elevated GGT (111 U/L)
- Standard Lipid Panel: Mildly elevated Total Cholesterol, elevated LDL-C, low-normal HDL-C, and highly elevated Triglycerides and non-HDL-C
- Advanced Lipoprotein Panel: Highly elevated Apo B, LDL-P, & sdLDL-C; low Apo A-I, HDL-P, and HDL-2C
- Inflammatory Markers: Elevated Fibrinogen, hs-CRP, MPO, and Uric Acid; normal Lp-PLA2
- Genetic Markers: Heterozygous MTHFR A1298C genotype (A/C); normal MTHFR C677T genotype (C/C); normal Apo E genotype (3/3)
- Nutritional Status Markers: Low Vitamin D and Omega-3 Index, borderline-low Vitamin B12 and RBC Folate, elevated Homocysteine, borderline-high Ferritin; normal serum Iron
- Comprehensive Diabetes Panel: Borderline-high Fasting Glucose and Hemoglobin A1C, highly elevated Fasting Insulin; very low Adiponectin
- Sex Hormones: Low Testosterone; normal DHEA-S
Three Main Therapeutic Approaches
- Clinical nutrition
- Healthy lifestyle modification & physical activities
- Personalized nutritional supplementation program
Treatment Goals
- Reduce weight
- Increase energy
- Normalize lipid abnormalities
- Regulate blood sugar levels & prevent diabetes
- Reduce chronic inflammation (eg, elevated Fibrinogen, hs-CRP, MPO, Uric acid, & Homocysteine)
- Optimize nutritional/hormone status
Clinical Nutrition
General Guidelines
The patient was self-employed and had a busy lifestyle. He had little time and usually ate very little in the morning. As a result, I recommended that he start drinking a high-quality protein drink for breakfast, specifically a chocolate whey protein powder formula (20 g protein per scoop, and sweetened with stevia). I recommended that he add 1 scoop of the protein powder into a 26-oz bottle blender and mix with 2 tbsp chia seeds, 3-4 oz unsweetened organic almond milk, and filtered water. He was to shake the bottle well and slowly drink the mixture for 2-3 hours in the AM. This makes for an easy but healthy breakfast, and whey protein (especially with chocolate) has been shown to enhance weight loss, increase satiety, improve lipid/metabolic syndrome parameters, and improve lean body mass.1,2 Since the drink reminded the patient of chocolate milk, he also liked the taste.
In addition to the breakfast recommendation, I also gave him the following general healthy eating guidelines, including foods to avoid and to consume. In general, I recommended that he concentrate on lean animal protein and leafy vegetables, and attempt to avoid all processed starchy carbohydrates.
- Eat real, unprocessed, whole, fresh, local, and organic foods. Examples include fresh vegetables and fruits, whole grains, beans, nuts, seeds, lean animal protein (eg, small wild fish, chicken, turkey, eggs). If fresh vegetables are not available, frozen vegetables are fine. However, NEVER use canned vegetables, which contain minimal or no essential nutrients; the can lining may also contain BPA (bisphenol A) or other BPA substitutes that can disrupt hormones.
- Choose the right carbs. Consume mainly leafy vegetables (at least 5 servings per day – each serving is 1 cup of raw vegetables), such as kale, collard greens, spinach, bok choy, chard, asparagus, Brussels sprout, broccoli, etc. Limit total starch intake to less than 2 cups of cooked starch daily. Starches can come from starchy vegetables (eg, root vegetables and squashes), all types of grains, and beans/lentils.
- Limit fruit intake to 1 serving daily, and avoid high-sugar fruits (eg, melons, grapes, banana, pineapple). Also avoid all fruit juices, which contain mostly sugars.
- Consume healthy snacks from nuts & seeds (no more than 1 cup daily). Healthy nuts include unsalted almonds, walnuts, pistachios, and Brazil nuts. Healthy seeds include pumpkin seeds and sunflower seeds. You may also consume an additional 2 tbsp of chia seeds daily to raise daily fiber intake, improve digestive system, increase satiety, regulate blood sugar levels, and reduce cholesterol.
- AVOID regular & diet soda, which can negatively affect body weight as well as blood glucose, triglycerides, and insulin levels
- Read food labels! Avoid any synthetic food colorings (eg, FD&C Red#40, Yellow #6, Yellow #5, Blue #1), artificial flavors (eg, MSG), artificial sweeteners (eg, sucralose, aspartame, acesulfame potassium, etc), preservatives (eg, sodium benzoate)
Foods to Avoid
The goals in avoiding the following foods included normalizing cholesterol, reversing insulin resistance, promoting weight loss, and optimizing overall health:
- Saturated fats (eg, cheeses, deep-fried foods, butter, margarine, beef, pork fat, chicken skin, etc)
- Refined or simple carbohydrates, which increase triglycerides (eg, white flour, white rice, white bread, white potato, white pasta, high-fructose corn syrup, any fruit juices or other sweet drinks, candy bars, pastries, candies, etc)
- Processed foods, including all trans fats and any hydrogenated oils; sugars, including table sugar, raw/brown sugar, maple syrup, and artificial sweeteners (eg, aspartame). Natural alternatives for sweeteners include stevia, monk fruit, and xylitol.
Foods to Consume
- High-fiber foods, including legumes, leafy green vegetables and salads, healthy unsalted nuts (eg, raw almonds, walnuts, pecans, pistachios, Brazil nuts, etc), healthy unsalted seeds (eg, pumpkin seeds, sunflower seeds, chia seeds, and ground flaxseeds). Gradually increase dietary fiber intake to 30-50 g/day)
- Anti-inflammatory omega-3 foods (eg, low-mercury fish, such as wild-caught salmon, sardines, and herring)
- Lean & high-quality protein sources (eg, legumes, organic grass-fed poultry, low-mercury fish, organic free-range eggs, healthy nuts and seeds). Also consume foods containing healthy fats, including avocados, almonds, walnuts, sesame seeds, coconut, and extra-virgin olive oil.
Healthy Lifestyle Modification & Physical Activities
Exercise
Make sure to engage in a regular exercise routine – both aerobic and strength-training exercises – to increase “healthy” cholesterol, ie, HDL-C, to improve the quality of cholesterol particles (specifically the particle size of both good and bad cholesterol fractions), and to support the cardiovascular system and prevent heart disease.
- Strength-training exercises (3 times weekly or every other day) help to maintain and build muscle mass, which helps normalize blood sugar levels, optimize body weight, and support energy metabolism. You can build your muscles in various ways, using everything from dumbbells to exercise bands, medicine balls, exercise machines, even your own body weight through martial arts, yoga, or Pilates. Aerobic exercise is also crucial for your health, since it exercises the heart. This should be a minimum of 30 minutes (4-5 times weekly) of brisk walking, biking, hiking, or swimming, or playing sports such as soccer, basketball, tennis, etc.
Sleep
Make sure to get enough sleep and rest nightly.
- Lack of sleep or poor sleep damages metabolism, promotes cravings for sugar and carbohydrates, makes you eat more, and drives up your risk of heart disease, diabetes, dementia, and early death. Ideally, you should go to bed no later than 10 PM and get up around 6 AM – for a total of 8 hours of sleep. Try to sleep at the same time every night (even on the weekends) to avoid stressing your body. Irregular sleep habits can disrupt your endocrine system, especially the stress hormone cortisol. When the body is under stress, adrenal glands secrete excessive cortisol, which induces glucose production and can eventually contribute to diabetes, dementia, and heart disease.
Personalized Nutritional Supplementation Program
In this case study, my main therapeutic goals for the nutritional supplements were to normalize lipids, reverse insulin resistance, reduce inflammatory markers, optimize nutritional/hormonal status, increase energy, and to enhance weight loss. The patient understood the treatment plan and was very compliant. He wanted to work with the treatment plan for 6 months before we reviewed his progress with repeat lab work. Below is my list of recommended nutritional supplements and the rationale for each.
- Berberine – 400 mg
- 1 capsule TID with food
- Berberine, an isoquinoline plant alkaloid, has been shown to safely improve metabolic syndrome/insulin resistance, lower triglycerides, reduce inflammation, and normalize atherogenic lipid particles3-5
- A berberine-containing formula (400-500 mg/capsule) ideally should contain alpha-lipoic acid (ALA) – at least 100 mg/capsule – which has been shown to improve lipids and insulin resistance markers6,7 The formula I recommended to the patient was a combination of berberine and ALA.
- Red Yeast Rice
- 1200 mg BID
- Red yeast rice (RYR), a traditional Chinese food, made by fermenting rice with Monascus purpureus, contains a bioactive component monacolin K, which acts like statin drugs (inhibition of HMG-CoA reductase) but without the side effects. Several studies have shown that RYR can significantly improve MetSyn by lowering cholesterol levels and that it possesses anti-inflammatory, anti-hypertensive, and anti-diabetic properties.4,8,9
- In this case, I recommended the RYR product that already contains coenzyme Q10 (80-100 mg/d), since RYR can potentially deplete coenzyme Q10 due to its statin-like property. Daily supplementation of 100 mg coenzyme Q10 can effectively decrease some pro-inflammatory factors, such as IL-6 and hs-CRP, and increase adiponectin.10
- Omega-3 Fish Oil (EPA + DHA) – 1000 mg of total omega-3s per capsule
- 1 capsule TID with food, or 3000 mg total omega-3s daily with food
- Omega-3 fish oil has been shown to prevent and improve metabolic syndrome11-13
- Probiotics (eg, Lactobacilli & Bifidobacteria) – 100 billion CFU per capsule
- I recommended that the patient take 1 capsule of probiotics daily after dinner
- The gut microbiome contributes approximately 2 kg of the whole body weight, and several studies suggest that gut microbiota has a profound effect on human metabolism, body weight, blood sugar regulation, immune modulation, and insulin sensitivity.14-17
- High-Quality & High-Potency Multivitamin
- The dosage of a high-quality, high-potency multivitamin formula I recommended to this patient was 1 capsule BID with meals
- Due to his poor dietary habits and MetSyn, I recommended that he take a high-quality multivitamin formula that also contained various vitamins and minerals, especially chromium and selenium. Researchers have found that patients with MetSyn tend to have lower levels of these minerals.18-20
- Natural B-Complex Formula (including folate, vitamins B2, B6, and B12) with N-Acetylcysteine (NAC)
- I recommended these nutrients because of the patient’s elevated level of Homocysteine (inflammatory byproduct that can negatively affect the cardiovascular system and the brain). Researchers have shown a beneficial effect of B vitamins on the prevention of MetSyn, as well as an inverse relationship between MetSyn and B vitamin levels.21-23
- Vitamin D3
- Due to the patient’s vitamin D deficiency status, I recommended that he take 10 000 IU vitamin D3 daily with food. Vitamin D deficiency has been associated with several chronic health issues, including MetSyn.24-27
- The vitamin D formula I recommended also contains vitamin K1 (phytonadione 200 µg) and vitamin K2 (menaquinone 720 µg), which can help distribute absorbed calcium into the bone (thereby strengthening it) and prevent calcium deposition in the walls of arteries (thereby reducing risk of atherosclerosis)
Lab Results – 6 Months Post-Treatment
Standard Lipid Panel
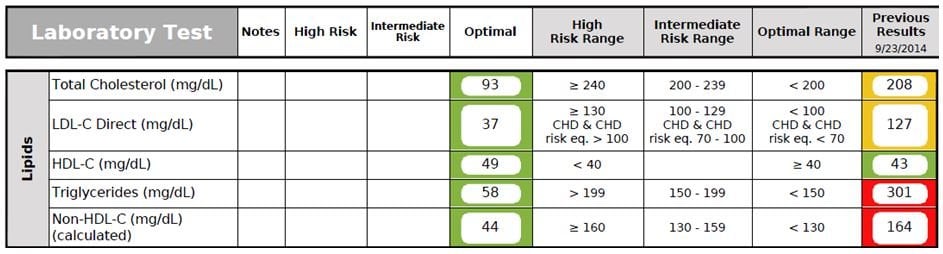
Figure 1. Standard Lipid Panel
Comment: The traditional lipid panel showed all normal results, including significant improvements in his Triglycerides, LDL-C, and non-HDL-C levels.
Advanced Lipoprotein Panel
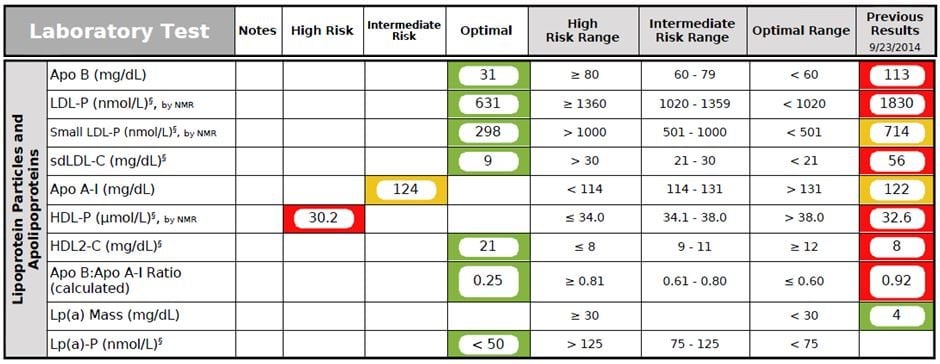
Figure 2. Advanced Lipoprotein Panel
Comment: The overall advanced lipid parameters showed significant improvements, especially Apo B, LDL-P, small LDL-P, sdLDL-C, and HDL2-C levels.
Inflammatory & Oxidative Stress Biomarkers
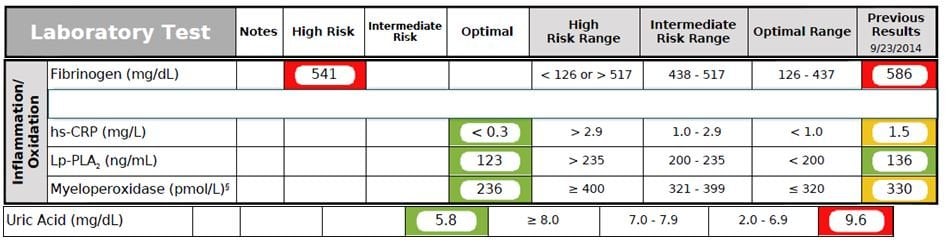
Figure 3. Inflammation/Oxidation Panel
Comment: The patient’s Fibrinogen level had improved but was still elevated. The rest of the inflammatory markers (hs-CRP, Lp-PLA2, MPO, and uric acid) also improved and were at optimal levels.
Liver Panel
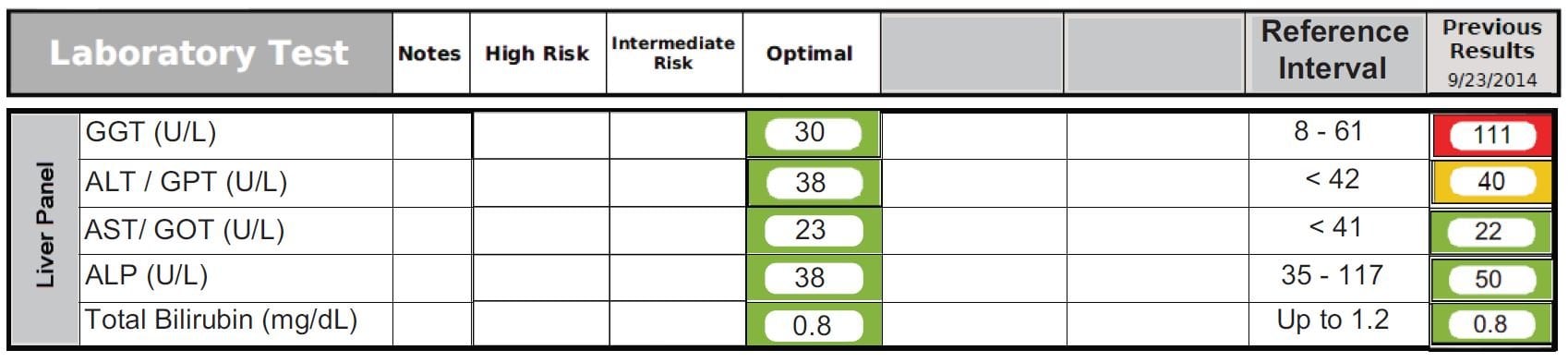
Figure 4. Liver Panel
Comment: The patient’s GGT level improved and was now at the optimal level. His ALT level improved but was still borderline-high.
Nutritional Status Biomarkers
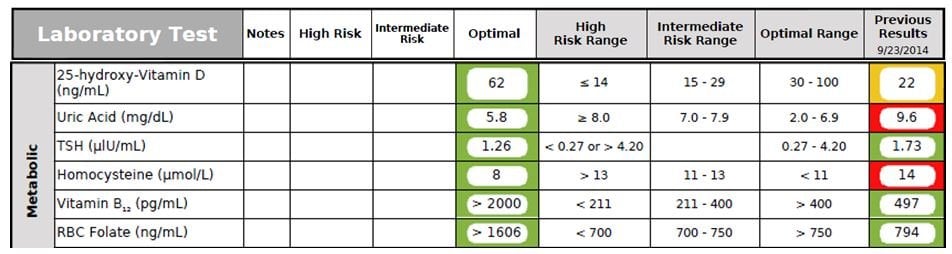
Figure 5. Nutritional Status Biomarkers
Comment: The patient’s Vitamin D, Uric cid, Homocysteine, Vitamin B12, and RBC Folate all improved and were at optimal levels.
RBC Omega-3 Index

Figure 6. Omega-3 Index
Comment: His Omega-3 Index improved and was at an optimal level.
Comprehensive Diabetes Panel

Figure 7. Diabetes Panel
Comment: The patient’s fasting Glucose and fasting Insulin significantly improved and were at optimal levels. The Adiponectin level improved as well.
Sex Hormones
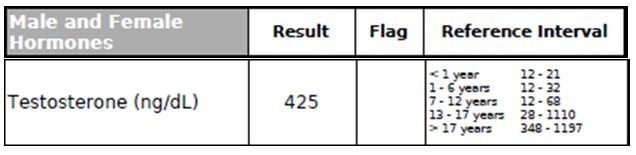
Figure 8. Testosterone
Comment: His Testosterone level improved (previous result 188 ng/dL), now at an optimal level (>400 ng/dL).
Summary
Using the personalized naturopathic treatment plan described above, the patient was able to lose 75 lb (from 230 lb to 155 lb) over a 6-month period. His lipid parameters normalized without the use of any prescribed medications. His inflammatory markers also normalized, except for Fibrinogen (although it improved). In terms of his liver panel, the GGT level normalized, and the ALT level improved but was still borderline-high after 6 months. All of his nutritional status markers (Vitamin D, Vitamin B12, Homocysteine, RBC Folate, and the Omega-3 Index) were optimized. His Adiponectin level also significantly improved but remained low. His Testosterone level was also optimized. Overall, the patient’s quality of life significantly improved. He reported having lots of energy and stamina, and has been very satisfied overall with the his results and experience.
As you can see in this case study, simple and healthy lifestyle changes using a personalized naturopathic nutritional supplementation program can be a powerful tool to essentially reverse metabolic syndrome and reduce risk of developing heart disease and diabetes within only a 6-month period. In this case, it also led to a remarkable improvement in quality of life for both the patient and his family.
References:
- Campbell CL, Foegeding EA, Harris GK. Cocoa and Whey Protein Differentially Affect Markers of Lipid and Glucose Metabolism and Satiety. J Med Food. 2016;19(3):219-227.
- Calton EK, James AP, Pannu PK, Soares MJ. Certain dietary patterns are beneficial for the metabolic syndrome: reviewing the evidence. Nutr Res. 2014;34(7):559-568.
- Pirillo A, Catapano AL. Berberine, a plant alkaloid with lipid- and glucose-lowering properties: From in vitro evidence to clinical studies. Atherosclerosis. 2015;243(2):449-461.
- McCarty MF, O’Keefe JH, DiNicolantonio JJ. Red Yeast Rice Plus Berberine: Practical Strategy for Promoting Vascular and Metabolic Health. Altern Ther Health Med. 2015;21 Suppl 2:40-45.
- Yao Z, Zhang L, Ji G. Efficacy of polyphenolic ingredients of Chinese herbs in treating dyslipidemia of metabolic syndromes. J Integr Med. 2014;12(3):135-146.
- Prieto-Hontoria PL, Pérez-Matute P, Fernández-Galilea M, et al. Effects of alpha-lipoic acid on chemerin secretion in 3T3-L1 and human adipocytes. Biochim Biophys Acta. 2016;1861(3):260-268.
- Chen WL, Kang CH, Wang SG, Lee HM. α-Lipoic acid regulates lipid metabolism through induction of sirtuin 1 (SIRT1) and activation of AMP-activated protein kinase. Diabetologia. 2012;55(6):1824-1835.
- Patel S. Functional food red yeast rice (RYR) for metabolic syndrome amelioration: a review on pros and cons. World J Microbiol Biotechnol. 2016;32(5):87.
- Ruscica M, Gomaraschi M, Mombelli G, et al. Nutraceutical approach to moderate cardiometabolic risk: results of a randomized, double-blind and crossover study with Armolipid Plus. J Clin Lipidol. 2014;8(1):61-68.
- Bagheri Nesami N, Mozaffari-Khosravi H, Najarzadeh A, Salehifar E. The Effect of Coenzyme Q10 Supplementation on Pro-Inflammatory Factors and Adiponectin in Mildly Hypertensive Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. Int J Vitam Nutr Res. 2015;85(3-4):156-164.
- Kim YS, Xun P, Iribarren C, et al. Intake of fish and long-chain omega-3 polyunsaturated fatty acids and incidence of metabolic syndrome among American young adults: a 25-year follow-up study. Eur J Nutr. 2016;55(4):1707-1716.
- Ahmadi A, Gharipour M, Arabzadeh G, et al. The effects of vitamin E and omega-3 PUFAs on endothelial function among adolescents with metabolic syndrome. Biomed Res Int. 2014;2014:906019.
- Cicero AF, Tartagni E, Ertek S. Nutraceuticals for metabolic syndrome management: from laboratory to benchside. Curr Vasc Pharmacol. 2014;12(4):565-571.
- Mazidi M, Rezaie P, Kengne AP, et al. Gut microbiome and metabolic syndrome. Diabetes Metab Syndr. 2016;10(2 Suppl 1):S150-S170.
- Stenman LK, Burcelin R, Lahtinen S. Establishing a causal link between gut microbes, body weight gain and glucose metabolism in humans – towards treatment with probiotics. Benef Microbes. 2015 Nov 13:1-12.
- Balasubramanian H, Patole S. Early probiotics to prevent childhood metabolic syndrome: A systematic review. World J Methodol. 2015;5(3):157-163.
- Goulet O. Potential role of the intestinal microbiota in programming health and disease. Nutr Rev. 2015;73 Suppl 1:32-40.
- Tükel HC, Alptekin Ö, Turan B, Delilbaşı E. Effects of metabolic syndrome on masseter muscle of male Wistar rats. Eur J Oral Sci. 2015;123(6):432-438.
- Wei J, Zeng C, Gong QY, et al. Associations between Dietary Antioxidant Intake and Metabolic Syndrome. PLoS One. 2015;10(6):e0130876.
- Galan P, Viteri FE, Bertrais S, et al. Serum concentrations of beta-carotene, vitamins C and E, zinc and selenium are influenced by sex, age, diet, smoking status, alcohol consumption and corpulence in a general French adult population. Eur J Clin Nutr. 2005;59(10):1181-1190.
- Bian S, Gao Y, Zhang M, et al. Dietary nutrient intake and metabolic syndrome risk in Chinese adults: a case-control study. Nutr J. 2013;12:106.
- Hildebrandt W, Sauer R, Bonaterra G, et al. Oral N-acetylcysteine reduces plasma homocysteine concentrations regardless of lipid or smoking status. Am J Clin Nutr. 2015;102(5):1014-1024.
- Kennedy DO. B Vitamins and the Brain: Mechanisms, Dose and Efficacy–A Review. Nutrients. 2016;8(2):68.
- Khaw KT, Luben R, Wareham N. Serum 25-hydroxyvitamin D, mortality, and incident cardiovascular disease, respiratory disease, cancers, and fractures: a 13-y prospective population study. Am J Clin Nutr. 2014;100(5):1361-1370.
- Rondanelli M, Perna S, Faliva M, et al. Focus on metabolic and nutritional correlates of polycystic ovary syndrome and update on nutritional management of these critical phenomena. Arch Gynecol Obstet. 2014;290(6):1079-1092.
- Hirani V, Cumming RG, Le Couteur DG, et al. Low levels of 25-hydroxy vitamin D and active 1,25-dihydroxyvitamin D independently associated with type 2 diabetes mellitus in older Australian men: the Concord Health and Ageing in Men Project. J Am Geriatr Soc. 2014;62(9):1741-1747.
- Wierzbicka J, Piotrowska A, Żmijewski MA. The renaissance of vitamin D. Acta Biochim Pol. 2014;61(4):679-686.
 Teerawong Kasiolarn, ND, MSAc, LAc, received his Doctorate of Naturopathic Medicine and Master of Science in acupuncture from Bastyr University in 2005. After graduation, he served as a naturopathic resident at UBCNM in CT, Yale-Prevention Research Center, and the Integrative Medicine Center at Griffin Hospital, a teaching facility affiliated with Yale University. For the 10 years since his residency, Dr Kasiolarn has been practicing at Nova Medical Group, the largest integrative primary care practice in Northern VA, as a naturopathic doctor and licensed acupuncturist. Dr Kasiolarn focuses on CVD, metabolic syndrome, diabetes, thyroid disorders, weight management/obesity, chronic pain, chronic fatigue, digestive disorders, anxiety/depression, and autoimmune diseases.
Teerawong Kasiolarn, ND, MSAc, LAc, received his Doctorate of Naturopathic Medicine and Master of Science in acupuncture from Bastyr University in 2005. After graduation, he served as a naturopathic resident at UBCNM in CT, Yale-Prevention Research Center, and the Integrative Medicine Center at Griffin Hospital, a teaching facility affiliated with Yale University. For the 10 years since his residency, Dr Kasiolarn has been practicing at Nova Medical Group, the largest integrative primary care practice in Northern VA, as a naturopathic doctor and licensed acupuncturist. Dr Kasiolarn focuses on CVD, metabolic syndrome, diabetes, thyroid disorders, weight management/obesity, chronic pain, chronic fatigue, digestive disorders, anxiety/depression, and autoimmune diseases.

















