

Male Health in Trouble?
John A. Robinson, NMD
Tolle Totum
The Global Decline in Testosterone and Sperm Count
Evidence suggests that testosterone and sperm levels are lowering in men across the globe.
Healthy, optimal serum levels of testosterone profoundly influence men’s health. Low testosterone levels are related to diseases such as cardiovascular disease,1 osteoporosis,2 Alzheimer’s disease,3 and diabetes.4 In addition, and less commonly known and appreciated, testosterone is responsible for healthy neurological function5 and improved psychosocial and behavioral dynamics.6
Research has begun to reveal a measurable decline in testosterone,7-9 as well as both sperm production7,10 and sperm quality,11,12 in men in industrialized countries across the world. Despite research that refuted the assertion of declining sperm,13,14 subsequent French research from 201315 again substantiated a decline, and even more recent research – in-depth meta-regression analysis from the Hebrew University-Hadassah Braun School of Public Health and Community Medicine and the Icahn School of Medicine at Mount Sinai16 – again argues for the original claim in the 1990s that sperm levels are indeed waning in many industrialized countries.
Evidence for Generational Testosterone Decline
It is generally understood that as American men age, total testosterone levels decline by about 1% annually, while free testosterone declines by about 2% annually.17 Additionally, a thorough 2007 analysis of data from the Massachusetts Male Aging Study (MMAS) by Travison et al demonstrated that population-level declines in testosterone over time are greater than the declines typically predicted by age.7 Evidence demonstrated that from the late 1980s through 2004, total and bioavailable testosterone decreased an average of 1.2% and 1.3%, respectively, when comparing one age cohort to another of the same age but from a different time period. For example, among men 65-69 years of age, average total testosterone levels fell from 503 ng/dL in 1988 to 423 ng/dL in 2003. This suggests that some factor other than age must be contributing to the declines in testosterone over time.
A recent study18 using data from the Third National Survey of Sexual Attitudes and Lifestyles (Natsal-3) concluded that there is an age-related decline in salivary testosterone levels in both men and women, which cannot be explained by an increase in ill health. The study perhaps offers some explanation for this trend, citing significant age-independent associations between lower salivary testosterone and higher body mass index (BMI), poorer self-reported general health, mobility problems, longstanding illness, and comorbid conditions such as cardiovascular disease and depression. Additional evidence of testosterone decline has been demonstrated in Finnish9 and Danish men.8
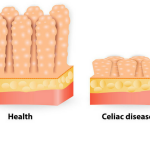
Evidence for Male Sperm Decline
Male Fertility Rates
The prevalence of infertility among couples is very high, affecting 1 in 7 couples in many countries; the most commonly identified cause is low sperm levels in males. Studies have shown that in young men 18-25 years of age, the prevalence of infertility is as high as 15-20%.19,20
The World Health Organization (WHO) defines infertility as “a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse.” According to the WHO, the overall prevalence of primary infertility ranges between 3.9% and 16.8%.21
Specifically in men, sperm analysis for fertility is broken down into various parameters. The WHO’s 5th edition of normal semen analysis values are listed below. It is important to note that these are minimal values and that many fertility specialists seek optimal levels that are higher than the WHO values. A mixture of normal, suboptimal, and/or frankly low measurements in any of these parameters can lead to a diagnosis of subfertility.
The Sperm Decline Controversy
Although several studies have suggested a decline in overall sperm quality over time, others have found no significant decline.13,14 The concern about declining sperm began in 1992 when Carlsen et al published a landmark meta-analysis of 61 studies, which found a significant global decline, between 1938 and 1991, in the average sperm concentration from 113 to 66 million/mL among men with no history of infertility.12 A scientific debate quickly ensued. However, 5 years later, Swan et al got involved, and after re-analyzing 56 studies, confirmed that a significant decline in sperm density had indeed occurred in the United States and Europe.22 In an extended meta-analysis of 101 studies, Swan et al again confirmed a decline in sperm density from 1934 to 1996.11 A 2013 French study by Rolland et al also concluded a trend of lowering sperm in their population.15
But the most recent study, by Levine et al in 2017,16 has hoisted the topic of sperm reduction into the mainstream, and has perhaps more definitively cemented the assertion that sperm is in a measurable decline. Using a regression meta-analysis – an elegant statistical model – they revealed a lowered sperm count and sperm concentration in men from North America, Europe, Australia, and New Zealand, from 1973 to 2011. Sperm concentration declined, on average, 1.4% per year, with an overall decline of 52.4%. The average decline in mean total sperm concentration was 1.6% per year, with an overall decline of 59.3%.16 It also appears that this trend is not slowing down, for when they limited their analysis to studies between 1995 and 2011, these declines were still evident.
Adding to the controversy, there are countries in which this global sperm decline is not apparent. Spain is one such example.23 In a study of 273 men from the Almeria region in Southern Spain, both semen count and testosterone levels were optimal and unchanged from November 2001 to December 2002. Spanish men have a low risk of testicular cancer in comparison to other European countries.24 The results of this study support the testicular dysgenesis syndrome (TDS) concept that suggests a link between impaired semen quality and testicular cancer risk.
Health Implications of Declining Sperm Count
Sperm and testosterone are inevitably physiologically related. Current scientific research along with clinical examination and monitoring should be considered for both of these parameters when determining overall health of a male patient. Levine’s introduction to his recent paper on declining sperm16 concisely summarizes the health implications and public health impact of declining sperm counts:
First, sperm count is closely linked to male fecundity and is a crucial component of semen analysis, the first step to identify male factor infertility. The economic and societal burden of male infertility is high and increasing. Second, reduced sperm count predicts increased all-cause mortality and morbidity. Third, reduced sperm count is associated with cryptorchidism, hypospadias and testicular cancer, suggesting a shared prenatal etiology. Fourth, sperm count and other semen parameters have been plausibly associated with multiple environmental influences, including endocrine disrupting chemicals, pesticides and lifestyle factors, including diet, stress, smoking and BMI. Therefore, sperm count may sensitively reflect the impacts of the modern environment on male health throughout the life course.
Health Implications of Low Testosterone
Cardiovascular Disease
Men show a higher incidence of cardiovascular disease than women, including myocardial infarction and stroke. Previously, it was assumed that because men have more testosterone than women, that the testosterone was to blame. This has been consistently challenged. Low testosterone is increasingly linked to risk of cardiovascular disease, and this is a current understanding.25,26 Even with regression analysis studies, it has been demonstrated that when the effects of such comorbid conditions are controlled for, the relationship between coronary artery disease and lower testosterone levels remains.27
Diabetes
The link between testosterone deficiency and type 2 diabetes mellitus is well known. Testosterone deficiency is common in adult type 2 diabetics, who also tend to show common symptoms of hypogonadism, such as sexual dysfunction and low libido.28
Obesity
A high BMI is related to lower testosterone levels. Several review studies support the notion that restoration of normal testosterone levels in obese men correlates with improved weight loss, reduction in waist circumference and BMI, and improvements in body composition including reduced body fat percentage and increased muscle mass.29-31 Additionally, a recent meta-analysis found that being overweight or obese was associated with a greater prevalence of azoospermia or oligozoospermia.32
Metabolic Syndrome
Metabolic Syndrome is defined by the International Diabetes Federation as having central obesity along with at least 2 of the following 4 abnormalities: hypertriglyceridemia, low HDL-cholesterol, hypertension, and high fasting blood sugar (or a previous diagnosis of type 2 diabetes). Various studies, including a 2014 meta-analysis, have shown metabolic syndrome to be highly associated with testosterone deficiency.33-35
Osteoporosis
The prevalence of male osteoporosis is very low under age 70, but rises significantly to an estimated prevalence of 22.6% in men >90 years old.36 Lifetime risk of fracture at ≥50 years of age is 50% for women and 20% for men.37,38 Testosterone positively affects bone growth and remodeling, and Late Onset Hypogonadism (LOH) has been related to bone loss in the aging male.39 Testosterone Replacement Therapy (TRT) to normalize testosterone serum blood levels has been shown to improve bone deposition and lower fracture risk.40,41
Age-Related Cognitive Decline
Testosterone has neuroprotective effects, including anti-inflammatory effects in the brain. Low testosterone levels in the aging male have been associated with both age-related cognitive decline and increased brain amyloid load, a major Alzheimer’s disease risk factor.42 TRT has been shown to improve cognition in older men.43
Depression & Anxiety
The aging male has an increased risk of depression and anxiety,44 the most common psychiatric disorders. Testosterone levels may play a role in this, since hypogonadal men have been shown to have an increased incidence of depression.45 TRT has been demonstrated to improve symptoms of depression,46 anxiety,47 and cognition48 in hypogonadal men.
Naturopathic & Functional Medicine Solutions
Indeed, the most poignant and utilitarian questions regarding declining testosterone or sperm counts are: What can we do about it? And, what should we do about it? And this is where the naturopathic physician excels – providing holistic and comprehensive medical solutions.
The research and general health implications associated with declining sperm and low testosterone that are discussed in this article is where we start. But the next step is doing what we do best: treating the whole person and providing excellent medical solutions that can heal the patient and influence the very fabric of society.
We must call on those specializing in men’s health within the naturopathic profession for continued leadership and imagination toward providing compelling and effective treatments.
I had the privilege to speak at the recent July 2017 meeting of the ICNM (International Congress on Naturopathic Medicine) in London, England, where this topic was presented before a large group of our international colleagues. The presentation was only weeks prior to the publication of Levine’s article on declining sperm counts.
In my companion paper49 to the London presentation, I offered several observations and calls to action, including interventions capable of stimulating testosterone, improving testicular function, sperm count and functionality, priming metabolism, and even promoting social change:
- Consistently monitor testosterone and sperm counts in a clinical observation setting, utilizing a functional approach that seeks to optimize clinical outcomes (as opposed to observation only with minimal clinical interventions).
- Continue to offer comprehensive, alternative options for male infertility services for pre-pregnant couples (clinical considerations for couple infertility often focuses on the female and considers the male secondarily).
- Maintain a clinical focus on the comorbid disorders associated with low testosterone and sperm count, including obesity, metabolic syndrome/diabetes, and cardiovascular disease. Additionally, continue to appreciate the association of lowering testosterone and sperm with the Testicular Dygenesis Syndrome (TDS), which includes hypospadias (the abnormal placement of the urethra on the penis), cryptorchidism (the condition of a missing testicle), and poor semen quality.
- Environmental toxicity and known Endocrine Disruptor Chemicals (EDCs) are likely one of the largest culprits in the generational decline of testosterone and sperm and the increasing risk of TDS. We must continue to be leaders in Environmental Medicine and to provide detoxification options for all.
- Continue to consider the medical option of comprehensive testosterone replacement therapy, when clinically appropriate and with consideration of the naturopathic Therapeutic Order.
- Turn toward a clinical view of testosterone replacement therapy that considers the “androgenicity” of the patient, ie, his complete physical and psychological presentation of testosterone expression. This includes considering the clinical end-point of the androgen receptor and its sensitivity, as opposed to simply the patient’s testosterone level in serum or saliva.
- Make botanical solutions readily available to physician and patient. Copious botanical solutions have been widely researched in studies that demonstrate their efficacy.
- When considering nutritional and dietary recommendations, bear in mind that multiple nutrients, particularly fat-soluble vitamins, are involved in both testosterone and sperm production. Also keep in mind that strict veganism can be detrimental to testosterone and sperm production and that the patient’s diet should contain adequate amounts of fat.
- Suggest exercises that include higher physical intensity with challenging weight loads in order to stimulate endocrine physiology and create metabolic demand for testosterone and sperm.
- Behavioral considerations might include increasing sexual activity (there is some suggestion that sexual contact is declining). Studies suggest that reduced sexual activity may compromise sperm quality50 and is inversely related to mortality.51 Also encourage engagement in fair competition among children and adults, such as in sports and academic achievements, as it facilitates testosterone production and androgen receptor sensitivity, particularly during development.
- Clinically consider the pregnant female, as evidence shows that the Testosterone Male is created by the Testosterone Female in utero. Optimal maternal testosterone levels will influence both the testosterone level and testosterone receptor sensitivity of the male fetus.
- Realize an appreciation for Behavioral Endocrinology and the updated scientific understanding that testosterone and its neurological and behavioral influence in fact yields stable, pro-social, assertive, self-reliant, competitive, and virile males – all necessary components of a healthy society.
References:
- Nettleship JE, Jones RD, Channer KS, Jones TH. Testosterone and coronary artery disease. Front Horm Res. 2009;37:91-107.
- Campion JM, Maricic MJ. Osteoporosis in men. Am Fam Physician. 2003;67(7):1521-1526.
- Moffat SD, Zonderman AB, Metter EJ, et al. Free testosterone and risk for Alzheimer disease in older men. Neurology. 2004;62(2):188-193.
- Barrett-Connor E. Lower endogenous androgen levels and dyslipidemia in men with non-insulin-dependent diabetes mellitus. Ann Intern Med. 1992;117(10):807-811.
- Celec P, Ostatníková D, Hodosy J. On the effects of testosterone on brain behavioral functions. Front Neurosci. 2015;9:12.
- Eisenegger C, Haushofer J, Fehr E. The role of testosterone in social interaction. Trends Cogn Sci. 2011;15(6):263-271.
- Travison TG, Araujo AB, O’Donnell AB, et al. A population-level decline in serum testosterone levels in American men. J Clin Endocrinol Metab. 2007;92(1):196-202.
- Andersson A, Jensen T, Juul A, et al. Secular decline in male testosterone and sex hormone binding globulin serum levels in Danish population surveys. J Clin Endocrinol Metab. 2007;92:4696-4705.
- Perheentupa A, Mäkinen J, Laatikainen T, et al. A cohort effect on serum testosterone levels in Finnish men. Eur J Endocrinol. 2013;168(2):227-233.
- Bhasin S. Secular decline in male reproductive function: Is manliness threatened? J Clin Endocrinol Metab. 2007;92(1):44-45.
- Swan SH, Elkin EP, Fenster L. The question of declining sperm density revisited: an analysis of 101 studies published 1934-1996. Environ Health Perspect. 2000;108(10):961-966.
- Carlsen E, Giwercman A, Keiding N, Skakkebaek NE. Evidence for decreasing quality of semen during past 50 years. BMJ. 1992;305(6854):609-613.
- Jouannet P, Wang C, Eustache F, et al. Semen quality and male reproductive health: the controversy about human sperm concentration decline. APMIS. 2001;109(5):333-344.
- Merzenich H, Zeeb H, Blettner M. Decreasing sperm quality: a global problem? BMC Public Health. 2010;10:24-24.
- Rolland M, Le Moal J, Wagner V, et al. Decline in semen concentration and morphology in a sample of 26,609 men close to general population between 1989 and 2005 in France. Hum Reprod. 2013;28(2):462-470.
- Levine H, Jørgensen N, Martino-Andrade A, et al. Temporal trends in sperm count: a systematic review and meta-regression analysis. July 25, 2017. Human Reproduction Update. Available at: https://academic.oup.com/humupd/article/doi/10.1093/humupd/dmx022/4035689/Temporal-trends-in-sperm-count-a-systematic-review. Accessed August 15, 2017.
- Feldman HA, Longcope C, Derby CA, et al. Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging study. J Clin Endocrinol Metab. 2002;87(2):589-598.
- Clifton S, Macdowall W, Copas AJ, et al. Salivary Testosterone Levels and Health Status in Men and Women in the British General Population: Findings from the Third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). J Clin Endocrinol Metab. 2016;101(11):3939-3951.
- Jørgensen N, Asklund C, Carlsen E, Skakkebaek NE. Coordinated European investigations of semen quality: results from studies of Scandinavian young men is a matter of concern. Int J Androl. 2006;29(1):54-61; discussion 105-108.
- Andersson AM, Jørgensen N, Main KM, et al. Adverse trends in male reproductive health: we may have reached a crucial ‘tipping point’. Int J Androl. 2008;31(2):74-80.
- Rutstein SO, Shah IH. Infecundity, Infertility, and Childlessness in Developing Countries. September 2004. DHS Comparative Reports No. 9. WHO Web site. http://www.who.int/reproductivehealth/topics/infertility/DHS-CR9.pdf. Accessed August 15, 2017.
- Swan SH, Elkin EP, Fenster L. Have sperm densities declined? A reanalysis of global trend data. Environ Health Perspect. 1997;105(11):1228-1232.
- Fernandez MF, Duran I, Olea N, et al. Semen quality and reproductive hormone levels in men from Southern Spain. Int J Androl. 2012;35(1):1-10.
- Bray F, Richiardi L, Ekbom A, et al. Trends in testicular cancer incidence and mortality in 22 European countries: continuing increases in incidence and declines in mortality. Int J Cancer. 2006;118(12):3099-3111.
- Rosano GM, Leonardo F, Pagnotta P, et al. Acute anti-ischemic effect of testosterone in men with coronary artery disease. Circulation. 1999;99(13):1666-1670.
- Malkin CJ, Pugh PJ, Morris PD, et al. Low serum testosterone and increased mortality in men with coronary heart disease. Heart. 2010;96(22):1821-1825.
- Njølstad I, Arnesen E, Lund-Larsen PG. Smoking, serum lipids, blood pressure, and sex differences in myocardial infarction. A 12-year follow-up of the Finnmark Study. Circulation. 1996;93(3):450-456.
- Putta S, Peluso I, Yarla NS, et al. Diabetes mellitus and male aging: Pharmacotherapeutics and clinical implications. Curr Pharm Des. 2017 Aug 22. doi: 10.2174/1381612823666170823103830. [Epub ahead of print]
- Traish AM. Testosterone and weight loss: the evidence. Curr Opin Endocrinol Diabetes Obes. 2014;21(5):313-322.
- Saad F, Yassin A, Doros G, Haider A. Effects of long-term treatment with testosterone on weight and waist size in 411 hypogonadal men with obesity classes I-III: observational data from two registry studies. Int J Obes (Lond). 2016;40(1):162-170.
- Saad F, Aversa A, Isidori AM, Gooren LJ. Testosterone as potential effective therapy in treatment of obesity in men with testosterone deficiency: a review. Curr Diabetes Rev. 2012;8(2):131-143.
- Sermondade N, Faure C, Fezeu L, et al. BMI in relation to sperm count: an updated systematic review and collaborative meta-analysis. Hum Reprod Update. 2013;19(3):221-231.
- Cunningham GR. Testosterone and metabolic syndrome. Asian J Androl. 2015;17(2):192-196.
- Wu FC, Tajar A, Beynon JM, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010;363(2):123-135.
- Brand JS, Rovers MM, Yeap BB, et al. Testosterone, sex hormone-binding globulin and the metabolic syndrome in men: an individual participant data meta-analysis of observational studies. PLoS One. 2014;9(7):e100409.
- [No authors listed]. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser. 1994;843:1-129.
- Melton LJ, Atkinson EJ, O’Connor MK, et al. Bone density and fracture risk in men. J Bone Miner Res. 1998;13(12):1915-1923.
- Melton JL. Perspectives: how many women have osteoporosis now? J Bone Miner Res. 1995;10(2):175-177.
- Mohamad NV, Soelaiman IN, Chin KY. A concise review of testosterone and bone health. Clin Interv Aging. 2016;11:1317-1324.
- Amory JK, Watts NB, Easley KA, et al. Exogenous testosterone or testosterone with finasteride increases bone mineral density in older men with low serum testosterone. J Clin Endocrinol Metab. 2004;89(2):503-510.
- Svartberg J, Agledahl I, Figenschau Y, et al. Testosterone treatment in elderly men with subnormal testosterone levels improves body composition and BMD in the hip. Int J Impot Res. 2008;20(4):378-387.
- Verdile G, Laws SM, Henley D, et al. Associations between gonadotropins, testosterone and beta amyloid in men at risk of Alzheimer’s disease. Mol Psychiatry. 2014;19(1):69-75.
- Bassil N, Alkaade S, Morley JE. The benefits and risks of testosterone replacement therapy: a review. Ther Clin Risk Manag. 2009;5(3):427-448.
- Khera M. Patients with testosterone deficit syndrome and depression. Arch Esp Urol. 2013;66(7):729-736.
- Shores MM, Sloan KL, Matsumoto AM, et al. Increased incidence of diagnosed depressive illness in hypogonadal older men. Arch Gen Psychiatry. 2004;61(2):162-167.
- Giltay EJ, Tishova YA, Mskhalaya GJ, et al. Effects of testosterone supplementation on depressive symptoms and sexual dysfunction in hypogonadal men with the metabolic syndrome. J Sex Med. 2010;7(7):2572-2582.
- Zhang XW, Liu ZH, Hu XW, et al. Androgen replacement therapy improves psychological distress and health-related quality of life in late onset hypogonadism patients in Chinese population. Chin Med J (Engl). 2012;125(21):3806-3810.
- Jung HJ, Shin HS. Effect of Testosterone Replacement Therapy on Cognitive Performance and Depression in Men with Testosterone Deficiency Syndrome. World J Mens Health. 2016;34(3):194-199.
- Robinson JA. The Global Decline of Testosterone & Sperm in the Western World: The Health, Social & Cultural Impact. Available at: http://www.hormone-zone.com/assets/docs/article.pdf. Accessed August 9, 2017
- Pellestor F, Girardet A, Andreo B. Effect of long abstinence periods on human sperm quality. Int J Fertil Menopausal Stud. 1994;39(5):278-282.
- Chen HK, Tseng CD, Wu SC, et al. A prospective cohort study on the effect of sexual activity, libido and widowhood on mortality among the elderly people: 14-year follow-up of 2,453 elderly Taiwanese. Int J Epidemiol. 2007;36(5):1136-1142.
Image Copyright: <a href=’https://www.123rf.com/profile_lightwise’>lightwise / 123RF Stock Photo</a>
 John A. Robinson, NMD, is a naturopathic medical doctor and author of 2 books: The Hormone Zone: Navigate Metabolism Towards Whole Health Transformation and ThyroZone: Real Thyroid Solutions for Better Health and Better Living. Dr Robinson, along with his wife and fellow naturopathic physician, Cristina Romero-Bosch, owns the cutting-edge medical center, The Hormone Zone. They are also Arizona’s medical leaders in Hormone Replacement Therapy, including Restorative and Sexual Regeneration Medicine. They have been serving thousands of men and women for over a decade. Follow them on Instagram @TheSexDocs and on Facebook at #TheHormoneZone.
John A. Robinson, NMD, is a naturopathic medical doctor and author of 2 books: The Hormone Zone: Navigate Metabolism Towards Whole Health Transformation and ThyroZone: Real Thyroid Solutions for Better Health and Better Living. Dr Robinson, along with his wife and fellow naturopathic physician, Cristina Romero-Bosch, owns the cutting-edge medical center, The Hormone Zone. They are also Arizona’s medical leaders in Hormone Replacement Therapy, including Restorative and Sexual Regeneration Medicine. They have been serving thousands of men and women for over a decade. Follow them on Instagram @TheSexDocs and on Facebook at #TheHormoneZone.







{kind=link}