

CBD Cases & Clinical Pearls: Anxiety & Depression
Integrative Cannabis
Aimée Gould Shunney, ND
Despite lightning-fast expansion of clinical use of hemp CBD (cannabidiol) in recent years, there is still a dearth of information available for healthcare practitioners (HCPs) that details the intricacies and pitfalls of recommending CBD in clinical practice. This article is not meant to describe the endocannabinoid system (ECS), CBD’s many mechanisms of action, or the latest research, some of which was illuminated in recent NDNR articles.1-3 Instead, it presents 3 case studies demonstrating how CBD can support anxiety, depression, and stress resilience, along with clinical pearls and lessons learned based on existing data and this naturopathic doctor’s experience. (See Table 1 for pre- and post-treatment summaries.)
Case Study 1
A 37-year-old female presented to the clinic with a 15-year history of anxiety and depression and associated panic attacks, for which she was prescribed sertraline, 100 mg daily. Prior to that, her anxiety was incapacitating and included sleep disturbance and social anxiety.
After beginning sertraline, she stated her symptoms improved by approximately 50%. She was started on full-spectrum hemp oil (FSHO) capsules containing 15 mg CBD, 2-3 times/day. Four weeks later, she reported her symptoms were approximately 60% reduced compared to using sertraline alone.
For the past year, she has also been able to maintain a reduced sertraline dose of 50 mg daily. The emotional blunting she attributed to the higher-dose sertraline was lessened with CBD. She noted increased self-confidence, improved job performance, and quality of her social life. Interestingly, she had comparable effects to the FSHO capsule when using a FSHO spray (containing 3 mg CBD per spray), 4 sprays 2-3 times/day, as well as a marijuana product (20:1 CBD:THC, standardized to 10 mg CBD/mL of tincture), 1 mL 2-3 times/day. She used these products separately, not together, and reported no adverse effects.
Case Study 2
A 49-year-old female presented with a history of anxiety, depression, and binge eating since early adulthood. She had been treated previously with various antidepressants, but not in 15 years. Symptoms began to worsen when caring for a sick child, and she began to experience tachycardia and palpitations related to anxiety that her sent to the emergency room on several occasions.
She was started on FSHO drops containing 2.5 mg CBD once daily, and she increased it to 2.5 mg twice daily after 2 weeks. (To get the approximate dose of 2.5 mg CBD, she used 7 drops of FSHO standardized to 5 mg CBD per 15 drops, or ½-dropperful.) Almost immediately, she reported a 60-70% reduction in her anxiety and depressive symptoms, and has had no further anxiety-related heart symptoms since starting on CBD 1 year ago. She reported feeling “dark and depressed” when she changed brands; however, this resolved by returning to the original product. She reports being more relaxed and that her family has noted significant improvement in her behavior as well. She has also experienced improved sleep and increased daytime energy. No adverse effects have been reported.
Case Study 3
A 54-year-old female presented with progressive anxiety and depression during perimenopause, which worsened with opiate use post-ACL injury, and worse from ongoing, severe familial stress. As her symptoms increased, she began to experience full-blown panic attacks. She was prescribed alprazolam, 0.25 mg to be used as needed, although she quickly increased the dose to 1-2 tablets daily. This felt unacceptable to her, however, in addition to leaving her tired and foggy.
She began a FSHO spray containing 3-9 mg CBD, which helped immediately during a panic attack in the office. For maintenance, she increased her CBD intake by taking a 25-mg CBD capsule daily with an additional 3-9 mg FSHO spray as needed.
After 1 month, she noted an approximate 50% reduction in her anxiety symptoms and has had no further panic attacks. She discontinued the alprazolam, and has been off of it for 2 years. In addition to improved sleep, she has had fewer symptoms of wheezing related to her asthma. She has experienced no adverse effects from the CBD or any withdrawal symptoms from stopping the alprazolam.
Table 1. Clinical Cases: Summaries
| BASELINE (BEFORE TREATMENT) | |||
| Case 1 | Case 2 | Case 3 | |
| Age/Sex | 37 y/o female | 49 y/o female | 54 y/o female |
| Diagnosis | Anxiety
Depression Panic attacks Social anxiety |
Anxiety
Depression Anxiety-related heart palpitations |
Anxiety
Depression Panic attacks |
| Symptom Scale (1-10) | 5/10 | 7-8/10 | 5-6/10 |
| Medications/Treatments per Day | Sertraline, 100 mg
Progesterone, 100 mg Fish oil |
Digestive enzymes; probiotic; olive leaf extract, oregano oil; vitamin D; herbal antihistamine | Alprazolam, 0.25 mg 2x/day
Fish oil; B-complex; multi-vitamin; broad-spectrum digestive support; probiotic |
| History of Cannabis Use | THC (5 mg) PRN, to help with sleep | None | High school marijuana use |
| POST-TREATMENT USING CBD* | |||
| Case 1 | Case 2 | Case 3 | |
| Symptom Scale
(1-10) |
1-2/10
No panic attacks |
2-4/10
No palpitations |
2-3/10
No panic attacks |
| Medications/Treatments per Day | Sertraline, 50 mg | None | None |
| Hemp CBD*
|
15 mg CBD capsule, 2-3x/day
OR 6 mg CBD spray, 2-3x/day OR Marijuana product (20:1 CBD:THC) standardized to 10 mg CBD/mL of tincture, 1 mL 2-3x/day |
2.5 mg CBD drops, 2x/day | 25 mg CBD capsule daily;
CBD spray PRN for breakthrough anxiety; 6-9 mg CBD spray PRN at bedtime to help with sleep |
*All products were FSHO (full-spectrum hemp oil), with the exception of the marijuana product in Case 1.
Clinical Considerations
Start Low, Go Slow
A titration schedule is an excellent way to begin using CBD (see Figure 1). Less is often more, and the schedule allows the patient (and HCP) to see this clearly. Too much CBD can lead to sedation.
Small amounts of CBD (3-10 mg) can sometimes manage anxiety and “stress overwhelm,” although 15-25 mg may be needed for daily anxiety. Larger amounts (25-50 mg+) are often required for pain and inflammation. Dosing can vary between patients with similar conditions, as can be seen with the patient in Case 2 requiring much smaller doses of CBD to manage her anxiety compared to the patient in Case 3. A recent case series reported a 79% improvement in anxiety with FSHO containing 25 mg CBD.4
Since CBD is fast-acting, it can be used as needed and for breakthrough anxiety. Sublingual use (whether spray or sublingual drops swished around the mouth for 30-60 sec) typically produce effects within 15-20 minutes, and oral products within 45-60 minutes, although data suggest it could take as long as 2 hours.5 As the ECS is modulated by CBD, and better tone being established as a result, patients will often find that they can use less CBD or stop altogether.
Figure 1. CBD Dosing: 14-Day Titration Schedule
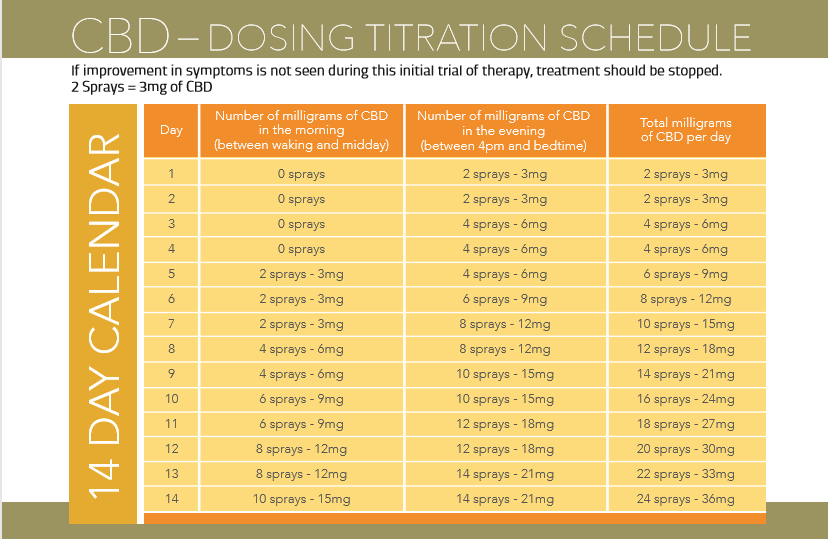
Adapted from chart by Sativex (http://sativex.co.uk/ms-nurses/dosing-and-titration/); permission for use was granted by CV Sciences.
Varied Results, Varied Products
CBD isolates are rarely used outside of the research arena. Most consumers use FSHOs or marijuana products, each varying in the profile of cannabinoids, terpenes, flavonoids, plant sterols, essential fats, etc. The cumulative benefits of this matrix were first described in 1998 as the entourage effect6 and, more recently in hemp circles, as the hemptourage effect. The variable matrix helps to explain why no product works for every person, as with the Case 2 patient who felt “spiritual and grounded” using one product, but “dark and depressed” with another. This is not uncommon. While our clinical focus is currently on CBD dose, there is the entire matrix of the plant to consider.7
Plant-Drug Interactions
CBD is a substrate and inhibitor of several cytochrome P450 enzymatic pathways, and therefore has the potential to interact with drugs that use those same routes for metabolism.8 Human data have shown interactions between CBD and antiepileptic drugs or warfarin (n=1).9,10 Common sense supports proceeding with caution when using CBD with potentially synergistic agents, ie, pain meds, antidepressants, anti-anxiety and sleep meds. It should be noted that a 2018 review of cannabinoid-drug interactions found that reported adverse drug reactions occurred with high-dose CBD isolates but not with FSHOs.11
Cases 1 and 3 describe CBD being used successfully to reduce or eliminate use of psychotropic medications. This is not always possible, and the addition of cannabinoids to medication should be undertaken in a stepwise fashion to avoid adverse effects. Likewise, weaning from psychotropic medications should always be done slowly and under HCP supervision.
Quality
Cannabis is a bio-accumulator, meaning that it can concentrate heavy metals, pesticides, and other toxins. Therefore, choose “gold level” supplement companies that list mg amounts of CBD per dose (not per bottle) and which provide data on raw materials used as well as QR codes and/or certificates of analysis from third-party batch-testing that measures toxic exposure as well as mold content and solvent residue. The US Hemp Authority is an excellent resource, and has thus far listed certified 13 hemp CBD companies, using their rigorous standards.12
Responders & Non-responders
There is an art to obtaining a positive response with cannabis. Using the patient examples in this article, one can see the variations in dosing and product selection that can yield anti-anxiety and antidepressant responses. Selecting the right product, with the right blend of cannabinoids and terpenes and at the right dose, takes time and clinical experience. Part of this relates to the fact that CBD is working, at least in part, by creating healthier endocannabinoid signaling and tone. Many factors contribute to the functioning of a person’s ECS: diet, lifestyle, history of trauma, drug and environmental exposure, medications, weight, comorbidities, genetics, and more. As we learn more about cannabis medicine and the ECS, we will be better able to individualize dosing regimens and products for different patient needs.
Supporting the ECS
A healthy ECS is crucial for optimal HPA axis function,13 and it has a significant influence on our experience of stress, anxiety, and mood. Many time-tested naturopathic recommendations can also optimize ECS health, including regular fish consumption (consider a fish or algae oil supplement to improve the omega 3:6 ratio14,15) and foods high in flavonoids and polyphenols (eg, fruits, vegetables, legumes), spices (saffron, turmeric, black pepper, oregano, cinnamon, and nutmeg), and coffee in moderation. Catechins from green tea have also been shown to support the ECS.16 Many lifestyle choices also support the ECS, such as high-intensity exercise, cold exposure, sleep hygiene, and all manner of stress management and relaxation activities,17-19 ie, time in nature, laughter, connection, intimacy, meditation, mindfulness-based stress reduction, acupuncture, massage, etc. In addition, recent data support a vital relationship between the ECS, vitamin D deficiency, and the microbiome,20,21 as well as between sex hormones and endocannabinoid production and tone.22-24
References:
- Bongiorno P. CBD for Mental Health. NDNR. 2018;14(11):19-20.
- Corroon J. CBD Use in the United States: A Cross-Sectional Study & Perspective. NDNR. 2018;14(9):1-3.
- Streisfeld R. Holistic Use of CBD for Acne. NDNR. 2019;15(4):23.
- Shannon S, Lewis N, Lee H, Hughes S. Cannabidiol in Anxiety and Sleep: A Large Case Series. Perm J. 2019;23:18-041. doi: 10.7812/TPP/18-041.
- Lucas CJ, Galettis P, Schneider J.The pharmacokinetics and the pharmacodynamics of cannabinoids. Br J Clin Pharmacol. 2018;84(11):2477–2482.
- Ben-Shabat S, Fride E, Sheskin T, et al. An entourage effect: inactive endogenous fatty acid glycerol esters enhance 2-arachidonoyl-glycerol cannabinoid activity. Eur J Pharmacol. 1998;353(1):23-31.
- MacCallum CA, Russo EB. Practical considerations in medical cannabis administration and dosing. Eur J Intern Med. 2018;49:12-19.
- Jiang R, Yamaori S, Takeda S, et al. Identification of cytochrome P450 enzymes responsible for metabolism of cannabidiol by human liver microsomes. Life Sci. 2011;89(5-6):165-170.
- Geffrey AL, Pollack SF, Bruno PL, Thiele EA. Drug–drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia. 2015;56(8):1246-1251.
- Grayson L, Vines B, Nichol K, et al. An interaction between warfarin and cannabidiol, a case report. Epilepsy Behav Case Rep. 2017;9:10-11.
- Project CBD. Project CBD Releases Educational Primer on Cannabinoid-Drug Interactions. Last revised January 14, 2019. Available at: https://www.projectcbd.org/sobre-cbd/cannabis-pharmacology/project-cbd-releases-educational-primer-cannabinoid-drug. Accessed April 18, 2019.
- US Hemp Authority. Certified Companies. 2019. Available at: https://www.ushempauthority.org/certified-companies. Accessed April 18, 2019.
- Gorzalka BB, Hill MN. Integration of Endocannabinoid Signaling into the Neural Network Regulating Stress-Induced Activation of the Hypothalamic-Pituitary-Adrenal Axis. In: Kendall D, Alexander S, eds. Behavioral Neurobiology of the Endocannabinoid System. Heidelberg, Germany: Springer-Verlag; 2009.
- Larrieu T, Layé S. Food for Mood: Relevance of Nutritional Omega-3 Fatty Acids for Depression and Anxiety. Front Physiol. 2018;9:1047.
- Lafourcade M, Larrieu T, Mato S, et al. Nutritional omega-3 deficiency abolishes endocannabinoid-mediated neuronal functions. Nat Neurosci. 2011;14(3):345-350.
- Korte G, Dreiseitel A, Schreier P, et al. Tea catechins’ affinity for human cannabinoid receptors. Phytomedicine. 2010;17(1):19-22.
- Gertsch J. Cannabimimetic phytochemicals in the diet – an evolutionary link to food selection and metabolic stress adaptation? Br J Pharmacol. 2017;174(11):1464-1483.
- Krott LM, Piscitelli F, Heine M, et al. Endocannabinoid regulation in white and brown adipose tissue following thermogenic activation. J Lipid Res. 2016;57(3):464-473.
- McPartland JM, Guy GW, Di Marzo V. Care and feeding of the endocannabinoid system: a systematic review of potential clinical interventions that upregulate the endocannabinoid system. PLoS One. 2014;9(3):e89566.
- Rousseaux C, Thuru X, Gelot A, et al. Lactobacillus acidophilus modulates intestinal pain and induces opioid and cannabinoid receptors. Nat Med. 2007;13(1):35-37.
- Guida F, Boccella S, Belardo C, et al. Altered gut microbiota and endocannabinoid system tone in vitamin D deficiency-mediated chronic pain. Brain Behav Immun. 2019 Apr 3. pii: S0889-1591(18)31247-9. doi: 10.1016/j.bbi.2019.04.006. [Epub ahead of print]
- Ney LJ, Matthews A, Bruno R, Felmingham KL. Modulation of the endocannabinoid system by sex hormones: Implications for posttraumatic stress disorder. Neurosci Biobehav Rev. 2018;94:302-320.
- Cui N, Wang L, Wang W, et al. The correlation of anandamide with gonadotrophin and sex steroid hormones during the menstrual cycle. Iran J Basic Med Sci. 2017;20(11):1268-1274.
- Sabatucci A, Simonetti M, Tortolani D, et al. Role of Steroids on the Membrane Binding Ability of Fatty Acid Amide Hydrolase. Cannabis Cannabinoid Res. 2019;4(1):42-50.
 Aimée Gould Shunney, ND, graduated from NUNM in 2001 and sees patients at Santa Cruz Integrative Medicine, in Santa Cruz, CA. She specializes in women’s health, bioidentical hormone balancing, and functional digestive issues. In addition to private practice, Dr Aimée has been a consultant and medical advisor to the natural products industry since 2011. She has been with CV Sciences, makers of PlusCBD Oil, since 2014. Website: www.drshunney.com
Aimée Gould Shunney, ND, graduated from NUNM in 2001 and sees patients at Santa Cruz Integrative Medicine, in Santa Cruz, CA. She specializes in women’s health, bioidentical hormone balancing, and functional digestive issues. In addition to private practice, Dr Aimée has been a consultant and medical advisor to the natural products industry since 2011. She has been with CV Sciences, makers of PlusCBD Oil, since 2014. Website: www.drshunney.com





{kind=link}